

Successful paediatric HIV treatment in rural primary care in Africa
- PMID: 19880392
- PMCID: PMC3181433
- DOI: 10.1136/adc.2009.169367
Successful paediatric HIV treatment in rural primary care in Africa
Abstract
Objective: Clinical outcomes of HIV-infected children on antiretroviral treatment (ART) in a decentralised, nurse/counsellor-led programme.
Design: Clinical cohort.
Setting: KwaZulu-Natal, South Africa.
Patients: HIV-infected children aged <or=15 years on ART, June 2004-2008.
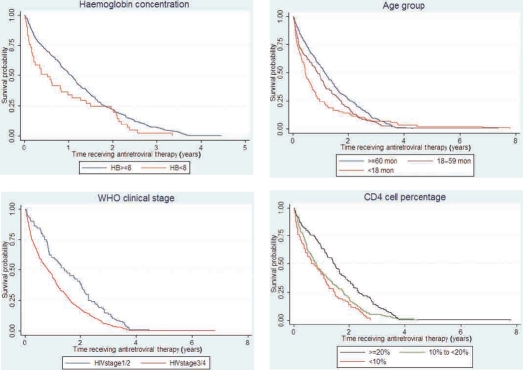
Main outcome measures: Survival according to baseline characteristics including age, WHO clinical stage, haemoglobin and CD4%, was assessed in Kaplan-Meier analyses. Hazard ratios for mortality were estimated using Cox proportional hazards regression and changes in laboratory parameters and weight-for-age z scores after 6-12 months' treatment were calculated.
Results: 477 HIV-infected children began ART at a median age of 74 months (range 4-180), median CD4 count (CD4%) of 433 cells/mm(3) (17%) and median HIV viral load of log 4.2 copies/ml; 105 (22%) were on treatment for tuberculosis and 317 (76.6%) were WHO stage 3/4. There were significant increases after ART initiation in CD4% (17% vs 22%; p<0.001), haemoglobin (9.9 vs 11.7 g/l; p<or=0.001) and albumin (30 vs 36 g/l; p<or=0.001). 32 (6.7%) children died over 732 child-years of follow-up (43.7 deaths/1000 child-years; 95% CI 32.7 to 58.2), 17 (53.1%) within 90 days of treatment initiation; median age of death was 84 (IQR 10-181) months. Children with baseline haemoglobin <or=8 g/l were more likely to die (adjusted HR 4.5; 95% CI 1.6 to 12.3), as were those aged <18 months compared with >60 months (adjusted HR 3.2; 95% CI 1.2 to 9.1).
Conclusions: Good clinical outcomes in HIV-infected children on ART are possible in a rural, decentralised service. Few young children are on ART, highlighting the urgent need to identify HIV-exposed infants.
Conflict of interest statement
Figures
References
-
- Bolton-Moore C, Mubiana-Mbewe M, Cantrell RA, et al. Clinical outcomes and CD4 cell response in children receiving antiretroviral therapy at primary health care facilities in Zambia. JAMA 2007;298:1888–99 - PubMed
-
- Fassinou P, Elenga N, Rouet F, et al. Highly active antiretroviral therapies among HIV-1-infected children in Abidjan, Côte d’Ivoire. AIDS 2004;18:1905–13 - PubMed
-
- O'Brien DP, Sauvageot D, Zachariah R, et al. In resource-limited settings good early outcomes can be achieved in children using adult fixed-dose combination antiretroviral therapy. AIDS 2006;20:1955–60 - PubMed
-
- Puthanakit T, Oberdorfer A, Akarathum N, et al. Efficacy of highly active antiretroviral therapy in HIV-infected children participating in Thailand's National Access to Antiretroviral Program. Clin Infect Dis 2005;41:100–7 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials