

Diagnosis and treatment of viral myocarditis
- PMID: 19880690
- PMCID: PMC2770911
- DOI: 10.1016/S0025-6196(11)60670-8
Diagnosis and treatment of viral myocarditis
Abstract
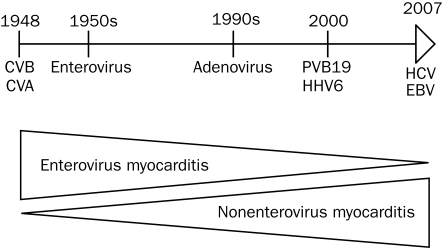
Myocarditis, an inflammatory disease of heart muscle, is an important cause of dilated cardiomyopathy worldwide. Viral infection is also an important cause of myocarditis, and the spectrum of viruses known to cause myocarditis has changed in the past 2 decades. Several new diagnostic methods, such as cardiac magnetic resonance imaging, are useful for diagnosing myocarditis. Endomyocardial biopsy may be used for patients with acute dilated cardiomyopathy associated with hemodynamic compromise, those with life-threatening arrhythmia, and those whose condition does not respond to conventional supportive therapy. Important prognostic variables include the degree of left and right ventricular dysfunction, heart block, and specific histopathological forms of myocarditis. We review diagnostic and therapeutic strategies for the treatment of viral myocarditis. English-language publications in PubMed and references from relevant articles published between January 1, 1985, and August 5, 2008, were analyzed. Main keywords searched were myocarditis, dilated cardiomyopathy, endomyocardial biopsy, cardiac magnetic resonance imaging, and immunotherapy.
Figures
References
-
- Klingel K, Sauter M, Bock CT, Szalay G, Schnorr JJ, Kandolf R. Molecular pathology of inflammatory cardiomyopathy. Med Microbiol Immunol. 2004May;193(2-3):101-117 Epub 2003 Aug 14 - PubMed
-
- Magnani JW, Danik HJ, Dec GW, Jr, DiSalvo TG. Survival in biopsy-proven myocarditis: a long-term retrospective analysis of the histopathologic, clinical, and hemodynamic predictors. Am Heart J. 2006;151(2):463-470 - PubMed
-
- Caforio AL, Calabrese F, Angelini A, et al. A prospective study of biopsy-proven myocarditis: prognostic relevance of clinical and aetiopathogenetic features at diagnosis. Eur Heart J. 2007June;28(11):1326-1333 Epub 2007 May 9 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
