

Radiological appearances of uterine fibroids
- PMID: 19881092
- PMCID: PMC2766886
- DOI: 10.4103/0971-3026.54887
Radiological appearances of uterine fibroids
Abstract
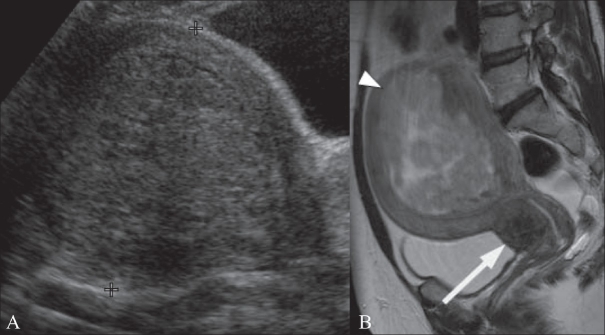
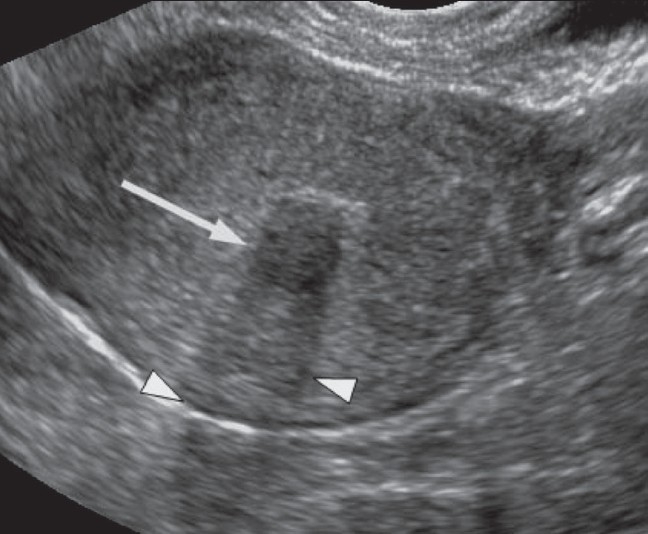
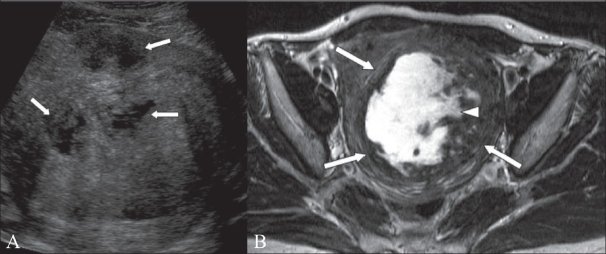
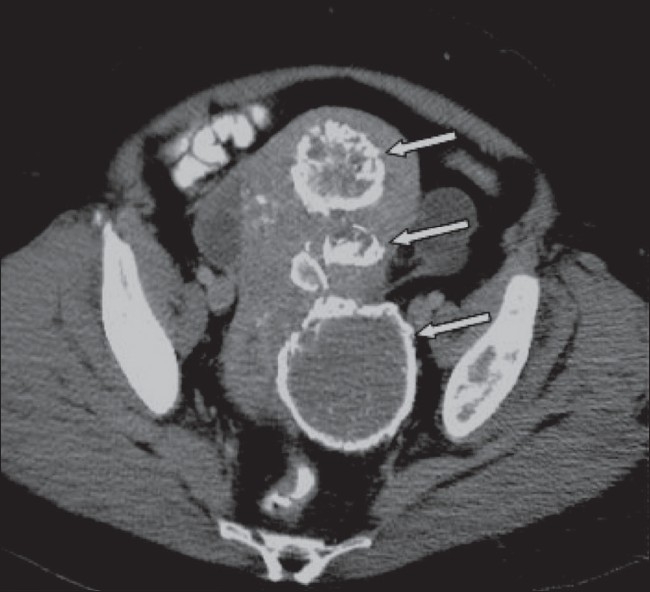
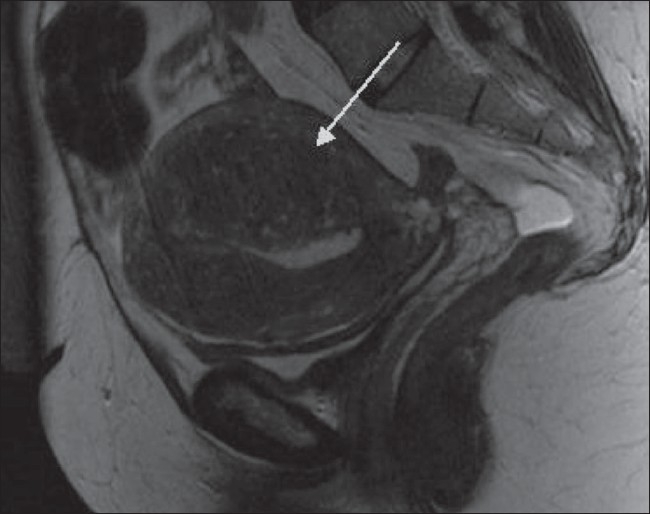
Uterine fibroids, also known as leiomyomas, are the commonest uterine neoplasms. Although benign, they can be associated with significant morbidity and are the commonest indication for hysterectomy. They are often discovered incidentally when performing imaging for other reasons. Usually first identified with USG, they can be further characterized with MRI. They are usually easily recognizable, but degenerate fibroids can have unusual appearances. In this article, we describe the appearances of typical and atypical uterine fibroids, unusual fibroid variants and fibroid mimics on different imaging modalities. Knowledge of the different appearances of fibroids on imaging is important as it enables prompt diagnosis and thereby guides treatment.
Conflict of interest statement
Figures
References
-
- Prayson RA, Hart WR. Pathologic considerations of uterine smooth muscle tumors. Obstet Gynecol Clin North Am. 1995;22:637–57. - PubMed
-
- Erdemoglu E, Kamaci M, Bayram I, Güler A, Güler SH Primary giant leiomyoma of the ovary – case report. Eur J Gynaecol Oncol. 2006;27:634–5. - PubMed
-
- Cramer SF. Patel A The frequency of uterine leiomyomas. Am J Clin Pathol. 1990;94:435–8. - PubMed
-
- Day Baird D, Dunson DB, Hill MC, Cousins D, Schectman J. High cumulative incidence of uterine leiomyoma in black and white women: Ultrasound evidence. Am J Obstet Gynecol. 2003;188:100–07. - PubMed
-
- Marshall LM, Spieglman D, Barbieri RL, Goldman MB, Manson JE, Colditz GA, Willett WC, Hunter DJ. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race. Obstet Gynecol. 1997;90:967–73. - PubMed
LinkOut - more resources
Full Text Sources
Medical