

Challenge and hope in radiotherapy of hepatocellular carcinoma
- PMID: 19881961
- PMCID: PMC2768232
- DOI: 10.3349/ymj.2009.50.5.601
Challenge and hope in radiotherapy of hepatocellular carcinoma
Abstract
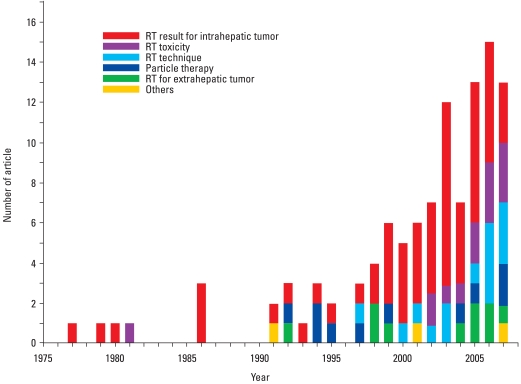
Hepatocellular carcinoma (HCC) is one of the most critical global health issues. With frequent association of viral liver disease, HCC is highly complex, harboring both cancer and chronic liver disease. The tumor stage and underlying liver function are both major determinants of the treatment selection as well as prognosis in HCC patients, thus allowing no more than a 20% chance for potentially curative therapies. Radiotherapy technology has been evolved remarkably during the past decade, and radiation can be precisely delivered, thereby permitting higher doses to the tumour and reduced doses to surrounding normal tissues. There has been increasing interest in the merits of radiotherapy in HCC over the past few years, as indicated by a Pub Med search. Radiotherapy has been used as the definitive therapy with curative intent in early stage tumours. It has been used also in combination with TACE for intermediate stage tumours. In locally advanced tumours, radiotherapy has been combined with systemic agents. Despite its efficacy, radiotherapy has not yet been incorporated into the standard management guidelines of HCC. The lack of high evidence level data, especially randomized controlled trials, has posed an obstacle in including radiotherapy into the routine treatment schema of HCC. Therefore, well-designed prospective studies are strongly recommended using developing technology for radiotherapy alone or combination therapies. Also, many issues such as the optimal dose-fractionation, intra- or extrahepatic metastasis after radiotherapy, and radiation-induced hepatic dysfunction remain to be solved. In this review, current status of radiotherapy for HCC will be discussed with regard to technical consideration and combination strategy. The limitation and future perspectives will also be discussed.
Keywords: Radiotherapy; hepatocellular carcinoma.
Conflict of interest statement
The author has no financial conflicts of interest.
Figures
References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Joo KR, Bang SJ, Song BC, Youn KH, Joo YH, Yang SH, et al. Hepatitis B viral markers of Korean adults in the late 1990s: survey data of 70,347 health screenees. Korean J Gastroenterol. 1999;33:642–652.
-
- Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology. 2004;127(5 Suppl 1):S5–S16. - PubMed
-
- Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001;35:421–430. - PubMed
-
- Bruix J, Sherman M Practice Guidelines Committee; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology. 2005;42:1208–1236. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
