

The surgical treatment for spinal intradural extramedullary tumors
- PMID: 19885053
- PMCID: PMC2766751
- DOI: 10.4055/cios.2009.1.3.165
The surgical treatment for spinal intradural extramedullary tumors
Abstract
Background: We wanted to investigate the results of surgical treatment and analyze the factors that have an influence on the neurologic symptoms and prognosis of spinal intradural extramedullary (IDEM) tumors.
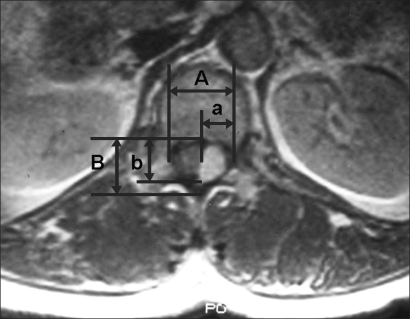
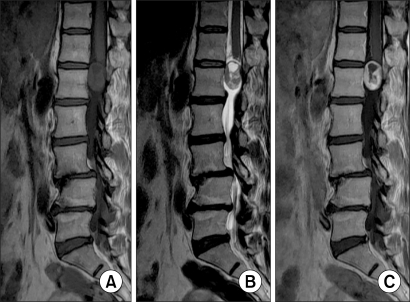
Methods: The spinal IDEM tumor patients (11 cases) who had been treated by surgical excision and who were followed up more than 1 year were retrospectively analyzed. Pain was evaluated by the visual analogue scale (VAS) and the neurologic function was assessed by Nurick's grade. The pathological diagnosis, the preoperative symptom duration, the tumor location on the sagittal and axial planes and the percentage of tumor occupying the intradural space were investigated. In addition, all these factors were analyzed in relation to the degree of the preoperative symptoms and the prognosis. On the last follow-up, the MRI was checked to evaluate whether or not the tumor had recurred.
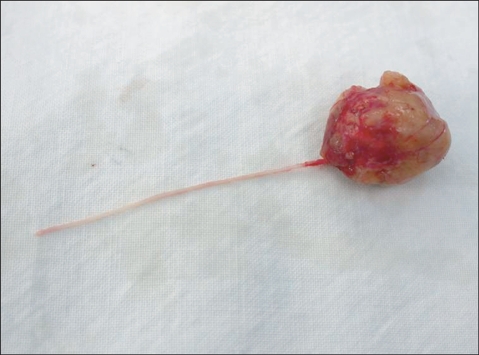
Results: The most common diagnosis was schwannomas (73%), followed by meningiomas (18%). The percentage of tumor occupying the intradural space was 82.9 +/- 9.4%. The VAS score was reduced in all cases from 8.0 +/- 1.2 to 1.2 +/- 0.8 (p = 0.003) and the Nurick's grade was improved in all cases from 3.0 +/- 1.3 to 1.0 +/- 0.0 (p = 0.005). The preoperative symptoms were correlated with only the percentage of tumor occupying the intradural space (VAS; r(2) = 0.75, p = 0.010, Nurick's grade; r(2) = 0.69, p = 0.019). One case of schwannoma recurred.
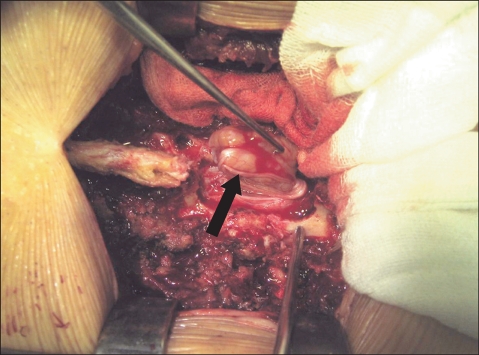
Conclusions: The degree of neurologic symptoms was correlated with the percentage of tumor occupying the intradural space. All the tumors were able to be excised through the posterior approach. The postoperative neurologic recovery was excellent in all the cases regardless of any condition. Therefore, aggressive surgical excision is recommended even for cases with a long duration of symptoms or a severe neurologic deficit.
Keywords: Intradural extramedullary tumor; Prognosis; Surgical treatment.
Figures

References
-
- Albanese V, Platania N. Spinal intradural extramedullary tumors: personal experience. J Neurosurg Sci. 2002;46(1):18–24. - PubMed
-
- el-Mahdy W, Kane PJ, Powell MP, Crockard HA. Spinal intradural tumours: Part I Extramedullary. Br J Neurosurg. 1999;13(6):550–557. - PubMed
-
- Tredway TL, Santiago P, Hrubes MR, Song JK, Christie SD, Fessler RG. Minimally invasive resection of intradural-extramedullary spinal neoplasms. Neurosurgery. 2006;58(1) Suppl:ONS52–ONS58. - PubMed
-
- Nurick S. The natural history and the results of surgical treatment of the spinal cord disorder associated with cervical spondylosis. Brain. 1972;95(1):101–108. - PubMed
-
- Helseth A, Mork SJ. Primary intraspinal neoplasms in Norway, 1955 to 1986: a population-based survey of 467 patients. J Neurosurg. 1989;71(6):842–845. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
