

Laboratory-based non-clinical comparison of occlusion rates using three rapid-acting insulin analogs in continuous subcutaneous insulin infusion catheters using low flow rates
- PMID: 19885209
- PMCID: PMC2769745
- DOI: 10.1177/193229680800200314
Laboratory-based non-clinical comparison of occlusion rates using three rapid-acting insulin analogs in continuous subcutaneous insulin infusion catheters using low flow rates
Abstract
Background: Rapid-acting analog insulin is used increasingly for continuous subcutaneous insulin infusion therapy (CSII). As the choice of insulin may be a determinant of catheter occlusion, we compared rates of early and late occlusion of a standard CSII catheter with three insulin analogs in a laboratory-based setting.
Methods: Twenty-four pumps were used for the study. Each insulin analog (glulisine, lispro, and aspart) was assigned to eight pumps in a randomized order for each of nine runs of 5-day duration. Pumps were primed to receive a basal dose of 0.1 IU/h with a bolus dose of 2 IU given three times each day. Pumps were placed in an incubator to maintain temperature in the range of 32 to 36 degrees C.
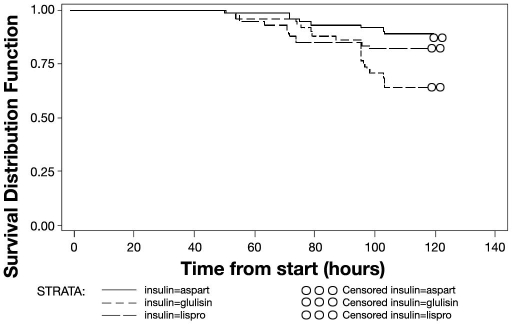
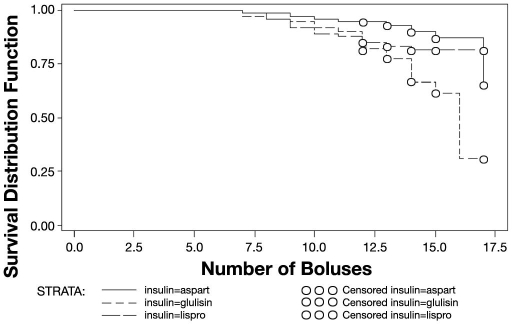
Results: Over the entire study period, there were 48 occlusions. Early occlusions (within 72 hours) occurred during five of the nine runs with no evidence of any difference between insulins (p = .27); there were no occlusions before 48 hours. Over the whole of the 5-day infusion period, the probabilities of overall occlusion for each insulin were 40.9% [28 to 55%, 95% confidence interval (CI)] for glulisine, 9.2% (4 to 19.5%, 95% CI) for aspart, and 15.7% (8.1 to 28.1%, 95% CI) for lispro. All occlusions, except for three, occurred during a bolus infusion.
Conclusions: During CSII under laboratory conditions, early catheter occlusions (within 72 hours) are rare and independent of the choice of insulin analog. For patients using insulin pump therapy, the importance of catheter change within 72 hours should be emphasized irrespective of the insulin used. Beyond 72 hours, the risk of occlusion differs between insulins, being more common with glulisine.
Keywords: CSII; analogs; insulin; occlusions; temperature.
Figures
References
-
- NICE Technology Appraisal Guidance No. 57: Guidance on the use of continuous subcutaneous insulin infusion for diabetes. National Institute for Clinical Excellence. 2003 Feb
-
- Plank J, Siebenhofer A, Berghold A, Jeitler K, Horvath K, Mrak P, Pieber TR. Systematic review and meta-analysis of short-acting insulin analogues in patients with diabetes mellitus. Arch Intern Med. 2005;165(12):1337–1344. - PubMed
-
- Medtronic Diabetes UK [homepage on the Internet] Watford UK: Medtronic MiniMed, Inc.; 2008. [cited 2007 September 30]. Effective infusion site management. Available from: http://www.medtronic-diabetes.co.uk/pdf/MedtronicUK/
-
- Guilhem I, Leguerrier AM, Lecordier F, Poirier JY, Maugendre D. Technical risks with subcutaneous insulin infusion. Diabetes Metab. 2006;32(3):279–284. - PubMed
-
- Weissberg-Benchell J, Antisdel-Lomaglio J, Seshadri R. Insulin pump therapy: a meta-analysis. Diabetes Care. 2003;26(4):1079–1087. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
