

Association of physical examination with pulmonary artery catheter parameters in acute lung injury
- PMID: 19885995
- PMCID: PMC4900681
- DOI: 10.1097/ccm.0b013e3181a59532
Association of physical examination with pulmonary artery catheter parameters in acute lung injury
Abstract
Objective: To correlate physical examination findings, central venous pressure, fluid output, and central venous oxygen saturation with pulmonary artery catheter parameters.
Design: Retrospective study.
Setting: Data from the multicenter Fluid and Catheter Treatment Trial of the National Institutes of Health Acute Respiratory Distress Syndrome Network.
Patients: Five hundred thirteen patients with acute lung injury randomized to treatment with a pulmonary artery catheter.
Interventions: Correlation of physical examination findings (capillary refill time >2 secs, knee mottling, or cool extremities), central venous pressure, fluid output, and central venous oxygen saturation with parameters from a pulmonary artery catheter.
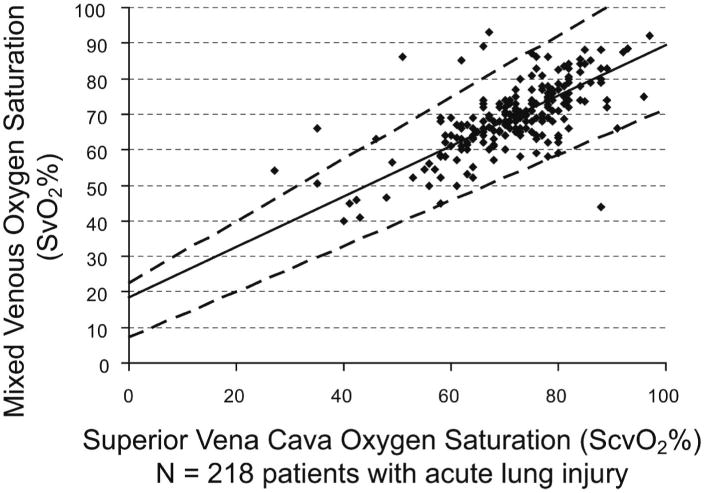
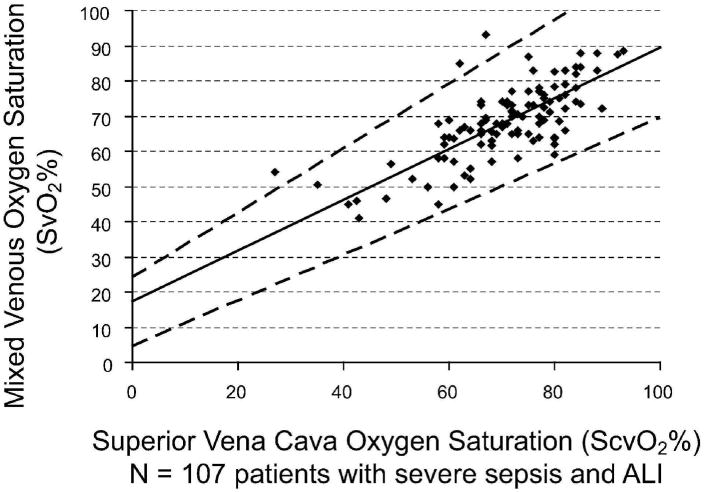
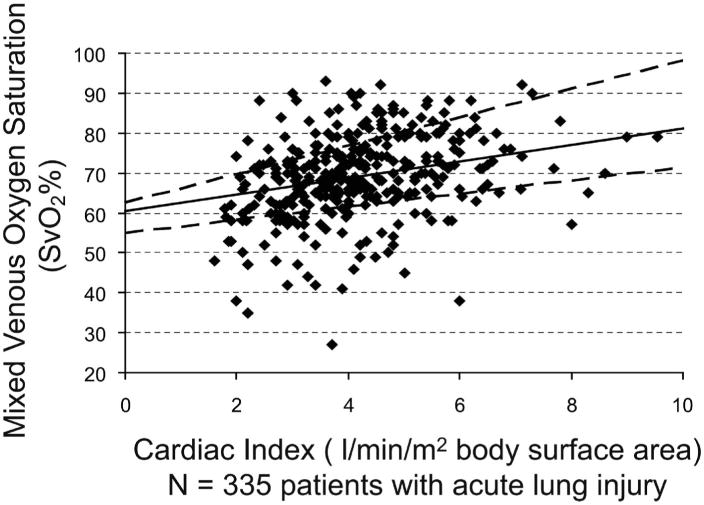
Measurements: We determined association of baseline physical examination findings and on-study parameters of central venous pressure and central venous oxygen saturation with cardiac index <2.5 L/min/m2 and mixed venous oxygen saturation <60%. We determined correlation of baseline central venous oxygen saturation and mixed venous oxygen saturation and predictive value of a low central venous oxygen saturation for a low mixed venous oxygen saturation.
Measurements and main results: Prevalence of cardiac index <2.5 and mixed venous oxygen saturation <60% was 8.1% and 15.5%, respectively. Baseline presence of all three physical examination findings had low sensitivity (12% and 8%), high specificity (98% and 99%), low positive predictive value (40% and 56%), but high negative predictive value (93% and 86%) for cardiac index <2.5 and mixed venous oxygen saturation <60%, respectively. Central venous oxygen saturation <70% predicted a mixed venous oxygen saturation <60% with a sensitivity 84%,specificity 70%, positive predictive value 31%, and negative predictive value of 96%. Low cardiac index correlated with cool extremities, high central venous pressure, and low 24-hr fluid output; and low mixed venous oxygen saturation correlated with knee mottling and high central venous pressure, but these correlations were not found to be clinically useful.
Conclusions: In this subset of patients with acute lung injury, there is a high prior probability that cardiac index and mixed venous oxygen saturation are normal and physical examination findings of ineffective circulation are not useful for predicting low cardiac index or mixed venous oxygen saturation. Central venous oxygen saturation <70% does not accurately predict mixed venous oxygen saturation <60%, but a central venous oxygen saturation >or=70% may be useful to exclude mixed venous oxygen saturation <60%.
Conflict of interest statement
The remaining authors have not disclosed any potential conflicts of interest.
Figures
Comment in
-
Pulmonary artery catheter redux: physical findings in acute respiratory distress syndrome/acute lung injury.Crit Care Med. 2009 Oct;37(10):2846-8. doi: 10.1097/CCM.0b013e3181b3a06a. Crit Care Med. 2009. PMID: 19865011 No abstract available.
References
-
- Harvey S, Harrison DA, Singer M, et al. Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): A randomised controlled trial. Lancet. 2005;366:472–477. - PubMed
-
- Richard C, Warszawski J, Anguel N, et al. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: A randomized controlled trial. JAMA. 2003;290:2713–2720. - PubMed
-
- Wheeler AP, Bernard GR, Thompson BT, et al. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med. 2006;354:2213–2224. - PubMed
-
- Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid—Management strategies in acute lung injury. N Engl J Med. 2006;354:2564–2575. - PubMed
-
- Gattinoni L, Brazzi L, Pelosi P, et al. A trial of goal-oriented hemodynamic therapy in critically ill patients. N Engl J Med. 1995;333:1025–1032. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
