

Predicting prognosis in hepatocellular carcinoma after curative surgery with common clinicopathologic parameters
- PMID: 19886989
- PMCID: PMC2785835
- DOI: 10.1186/1471-2407-9-389
Predicting prognosis in hepatocellular carcinoma after curative surgery with common clinicopathologic parameters
Abstract
Background: Surgical resection is one important curative treatment for hepatocellular carcinoma (HCC), but the prognosis following surgery differs substantially and such large variation is mainly unexplained. A review of the literature yields a number of clinicopathologic parameters associated with HCC prognosis. However, the results are not consistent due to lack of systemic approach to establish a prediction model incorporating all these parameters.
Methods: We conducted a retrospective analysis on the common clinicopathologic parameters from a cohort of 572 ethnic Chinese HCC patients who received curative surgery. The cases were randomly divided into training (n = 272) and validation (n = 300) sets. Each parameter was individually tested and the significant parameters were entered into a linear classifier for model building, and the prediction accuracy was assessed in the validation set
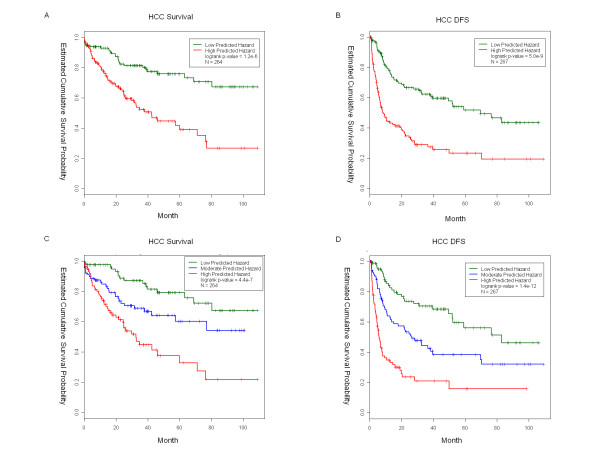
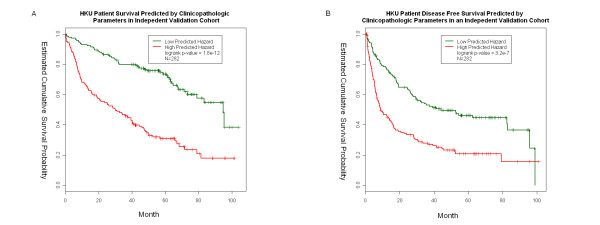
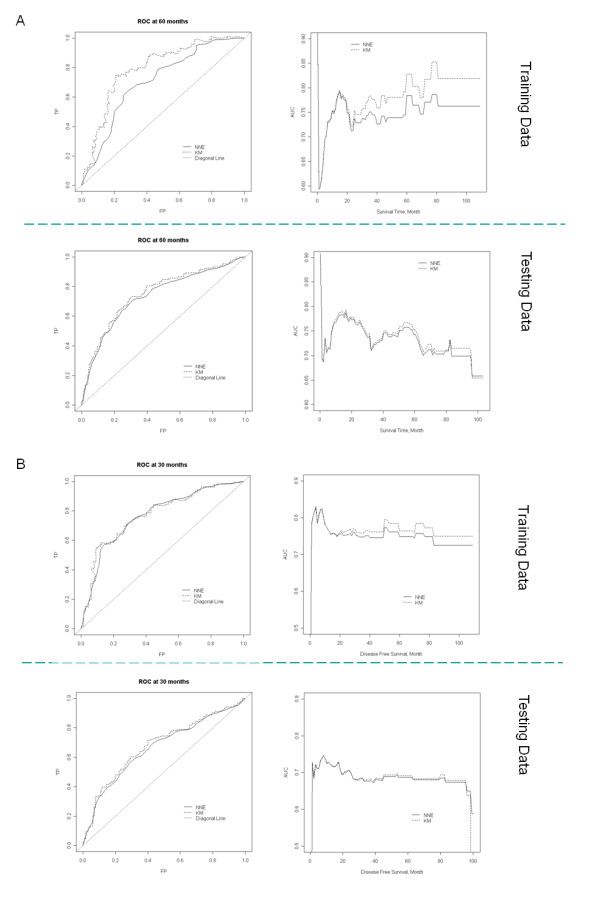
Results: Our findings based on the training set data reveal 6 common clinicopathologic parameters (tumor size, number of tumor nodules, tumor stage, venous infiltration status, and serum alpha-fetoprotein and total albumin levels) that were significantly associated with the overall HCC survival and disease-free survival (time to recurrence). We next built a linear classifier model by multivariate Cox regression to predict prognostic outcomes of HCC patients after curative surgery This analysis detected a considerable fraction of variance in HCC prognosis and the area under the ROC curve was about 70%. We further evaluated the model using two other protocols; leave-one-out procedure (n = 264) and independent validation (n = 300). Both were found to have excellent prediction power. The predicted score could separate patients into distinct groups with respect to survival (p-value = 1.8e-12) and disease free survival (p-value = 3.2e-7).
Conclusion: This described model will provide valuable guidance on prognosis after curative surgery for HCC in clinical practice. The adaptive nature allows easy accommodation for future new biomarker inputs, and it may serve as the foundation for future modeling and prediction for HCC prognosis after surgical treatment.
Figures
Similar articles
-
[A new prognostic score system of hepatocellular carcinoma following hepatectomy].Zhonghua Zhong Liu Za Zhi. 2017 Dec 23;39(12):903-909. doi: 10.3760/cma.j.issn.0253-3766.2017.12.005. Zhonghua Zhong Liu Za Zhi. 2017. PMID: 29262506 Chinese.
-
High level of intercellular adhesion molecule-1 affects prognosis of patients with hepatocellular carcinoma.World J Gastroenterol. 2015 Jun 21;21(23):7254-63. doi: 10.3748/wjg.v21.i23.7254. World J Gastroenterol. 2015. PMID: 26109813 Free PMC article.
-
Clinical and morpho-molecular classifiers for prediction of hepatocellular carcinoma prognosis and recurrence after surgical resection.Hepatol Int. 2019 Nov;13(6):715-725. doi: 10.1007/s12072-019-09978-9. Epub 2019 Sep 17. Hepatol Int. 2019. PMID: 31531761
-
Prognostic models for outcome prediction in patients with advanced hepatocellular carcinoma treated by systemic therapy: a systematic review and critical appraisal.BMC Cancer. 2022 Jul 9;22(1):750. doi: 10.1186/s12885-022-09841-5. BMC Cancer. 2022. PMID: 35810271 Free PMC article.
-
Imaging to Predict Prognosis in Hepatocellular Carcinoma: Current and Future Perspectives.Radiology. 2023 May;307(3):e221429. doi: 10.1148/radiol.221429. Epub 2023 Apr 4. Radiology. 2023. PMID: 37014244 Review.
Cited by
-
Cancer-associated carbohydrate antigens as potential biomarkers for hepatocellular carcinoma.PLoS One. 2012;7(7):e39466. doi: 10.1371/journal.pone.0039466. Epub 2012 Jul 13. PLoS One. 2012. PMID: 22808038 Free PMC article.
-
MiR-182 is up-regulated and targeting Cebpa in hepatocellular carcinoma.Chin J Cancer Res. 2014 Feb;26(1):17-29. doi: 10.3978/j.issn.1000-9604.2014.01.01. Chin J Cancer Res. 2014. PMID: 24653623 Free PMC article.
-
MicroRNA-4651 represses hepatocellular carcinoma cell growth and facilitates apoptosis via targeting FOXP4.Biosci Rep. 2020 Jun 26;40(6):BSR20194011. doi: 10.1042/BSR20194011. Biosci Rep. 2020. PMID: 32436934 Free PMC article.
-
DLK1-DIO3 genomic imprinted microRNA cluster at 14q32.2 defines a stemlike subtype of hepatocellular carcinoma associated with poor survival.J Biol Chem. 2011 Sep 2;286(35):30706-30713. doi: 10.1074/jbc.M111.229831. Epub 2011 Jul 7. J Biol Chem. 2011. PMID: 21737452 Free PMC article.
-
Gene signatures derived from a c-MET-driven liver cancer mouse model predict survival of patients with hepatocellular carcinoma.PLoS One. 2011;6(9):e24582. doi: 10.1371/journal.pone.0024582. Epub 2011 Sep 16. PLoS One. 2011. PMID: 21949730 Free PMC article.
References
-
- Bosch FX, Ribes J, Borras J. Epidemiology of primary liver cancer. Semin Liver Dis. 1999;19(3):271–285. - PubMed
-
- Kim JH, Choi MS, Lee H, Kim do Y, Lee JH, Koh KC, Yoo BC, Paik SW, Rhee JC. Clinical features and prognosis of hepatocellular carcinoma in young patients from a hepatitis B-endemic area. J Gastroenterol Hepatol. 2006;21(3):588–594. - PubMed
-
- Lam VW, Ng KK, Chok KS, Cheung TT, Yuen J, Tung H, Tso WK, Fan ST, Poon RT. Risk factors and prognostic factors of local recurrence after radiofrequency ablation of hepatocellular carcinoma. J Am Coll Surg. 2008;207(1):20–29. - PubMed
-
- Lau WY, Lai EC. Hepatocellular carcinoma: current management and recent advances. Hepatobiliary Pancreat Dis Int. 2008;7(3):237–257. - PubMed
-
- Sandhu DS, Tharayil VS, Lai JP, Roberts LR. Treatment options for hepatocellular carcinoma. Expert Rev Gastroenterol Hepatol. 2008;2(1):81–92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
