

Pancreatic pseudocysts: observation, endoscopic drainage, or resection?
- PMID: 19890418
- PMCID: PMC2770216
- DOI: 10.3238/arztebl.2009.0614
Pancreatic pseudocysts: observation, endoscopic drainage, or resection?
Abstract
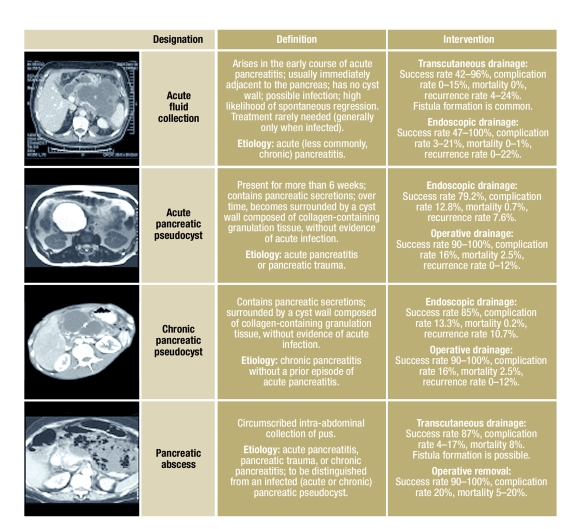
Background: Pancreatic pseudocysts are a common complication of acute and chronic pancreatitis. They are diagnosed with imaging studies and can be treated successfully with a variety of methods: endoscopic transpapillary or transmural drainage, percutaneous catheter drainage, laparoscopic surgery, or open pseudocystoenterostomy.
Methods: Relevant publications that appeared from 1975 to 2008 were retrieved from the MEDLINE, PubMed and EMBASE databases for this review.
Results: Endoscopic pseudocyst drainage has a high success rate (79.2%) and a low complication rate (12.9%). Percutaneous drainage is mainly used for the emergency treatment of infected pancreatic pseudocysts. Open internal drainage and pseudocyst resection are surgical techniques with high success rates (>92%), but also higher morbidity (16%) and mortality (2.5%) than endoscopic treatment (mortality 0.7%). Laparoscopic pseudocystoenterostomy, a recently introduced procedure, is probably similar to the endoscopic techniques with regard to morbidity and mortality.
Conclusions: An interdisciplinary approach is best suited for the safe and effective stage-specific treatment of pancreatic pseudocysts. The different interventional techniques that are currently available have yet to be compared directly in randomized trials.
Keywords: drainage; endoscopy; minimally invasive therapy; pancreatitis; spontaneous remission.
Figures
Comment in
-
Course and pathogenesis.Dtsch Arztebl Int. 2010 Jan;107(3):42; author reply 42. doi: 10.3238/arztebl.2010.0042a. Epub 2010 Jan 15. Dtsch Arztebl Int. 2010. PMID: 20140181 Free PMC article. No abstract available.
References
-
- Bradley EL., 3rd A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg. 1993;128:586–590. - PubMed
-
- Imrie CW, Buist LJ, Shearer MG. Importance of cause in the outcome of pancreatic pseudocysts. Am J Surg. 1988;156:159–162. - PubMed
-
- Maringhini A, Uomo G, Patti R, et al. Pseudocysts in acute nonalcoholic pancreatitis: incidence and natural history. Dig Dis Sci. 1999;44:1669–1673. - PubMed
-
- Barthet M, Bugallo M, Moreira LS, Bastid C, Sastre B, Sahel J. Management of cysts and pseudocysts complicating chronic pancreatitis. A retrospective study of 143 patients. Gastroenterol Clin Biol. 1993;17:270–276. - PubMed
-
- Ammann RW, Akovbiantz A, Largiader F, Schueler G. Course and outcome of chronic pancreatitis. Longitudinal study of a mixed medical-surgical series of 245 patients. Gastroenterology. 1984;86:820–828. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical