

Facial reconstruction by biosurgery: cell transplantation versus cell homing
- PMID: 19891541
- PMCID: PMC2867556
- DOI: 10.1089/ten.TEB.2009.0496
Facial reconstruction by biosurgery: cell transplantation versus cell homing
Abstract
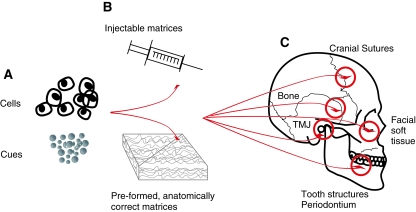
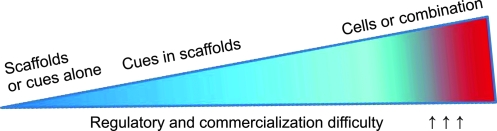
The face distinguishes one human being from another. When the face is disfigured because of trauma, tumor removal, congenital anomalies, or chronic diseases, the patient has a strong desire for functional and esthetic restoration. Current practice of facial reconstruction using autologous grafts, synthetic fillers, and prostheses is frequently below the surgeon's and patient's expectations. Facial reconstruction is yet to take advantage of recent advances in seemingly unrelated fields of stem cell biology, chemical engineering, biomaterials, and tissue engineering. "Biosurgery," a new concept that we propose, will incorporate novel principles and strategies of bioactive cues, biopolymers, and/or cells to restore facial defects. Small facial defects can likely be reconstructed by cell homing and without cell transplantation. A critical advantage of cell homing is that agilely recruited endogenous cells have the potential to harness the host's innate capacity for regeneration, thus accelerating the rate of regulatory and commercialization processes for product development. Large facial defects, however, may not be restorable without cell delivery per our understanding at this time. New breakthrough in biosurgery will likely originate from integrated strategies of cell biology, cytokine biology, chemical engineering, biomaterials, and tissue engineering. Regardless of cell homing or cell delivery approaches, biosurgery not only will minimize surgical trauma and repetitive procedures, but also produce long-lasting results. At the same time, caution must be exercised against the development of products that lack scientific basis or dogmatic combination of cells, biomaterials, and biomolecules. Together, scientifically derived biosurgery will undoubtedly develop into new technologies that offer increasingly natural reconstruction and/or augmentation of the face.
Figures
References
-
- U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health; 2000.
-
- Kim J. Zemnick C. Mao J.J. Restoration of oral and craniofacial defects by stem cells and bioengineering approaches. In: Nanda R., editor; Kapila S., editor. Science and Practice of Dentofacial Orthopedics. New York: Elsevier; 2009. pp. 134–149.
-
- Tanaka N. Uchide N. Suzuki K. Tashiro T. Tomitsuka K. Kimijima Y. Amagasa T. Maxillofacial fractures in children. J Craniomaxillofac Surg. 1993;21:289. - PubMed
-
- Karlson T.A. The incidence of facial injuries from dog bites. JAMA. 1984;251:3265. - PubMed
-
- Eastridge B.J. Owsley J. Sebesta J. Beekley A. Wade C. Wildzunas R. Rhee P. Holcomb J. Admission physiology criteria after injury on the battlefield predict medical resource utilization and patient mortality. J Trauma. 2006;61:820. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
