

Self-expanding stent for recanalization of acute embolic or dissecting intracranial artery occlusion
- PMID: 19892814
- PMCID: PMC7963979
- DOI: 10.3174/ajnr.A1865
Self-expanding stent for recanalization of acute embolic or dissecting intracranial artery occlusion
Abstract
Background and purpose: Stent placement may be an effective and last resort method for recanalization of recalcitrant intracranial artery occlusion. The purpose of this study was to evaluate the safety and efficacy of a self-expanding stent for the recanalization of acute embolic or dissecting intracranial artery occlusion.
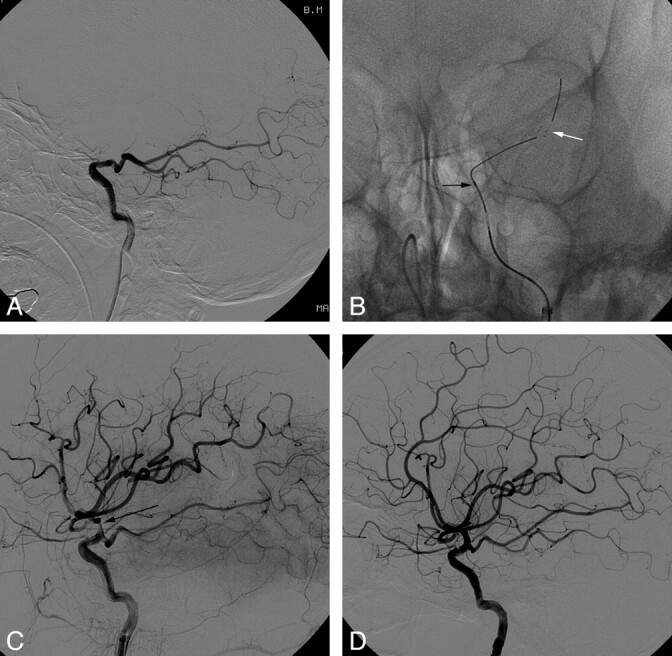
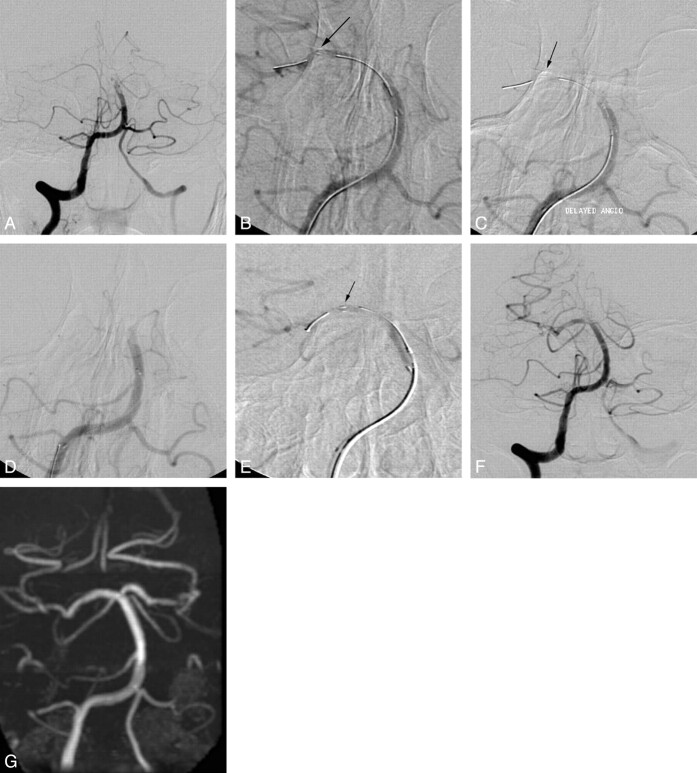
Materials and methods: Nine patients (mean age, 66 years; NIHSS score, 10-23) with acute embolic (n = 8) or dissecting occlusion (n = 1) of the intracranial arteries (ICA terminus in 5, MCA in 3, and BA in 1) were treated with a recapturable self-expanding stent. The safety and efficacy of the stent for recanalization were evaluated retrospectively.
Results: The emboli were entrapped against the vessel wall by the stent, resulting in immediate recanalization (TIMI 2) in all embolic occlusions. The dissecting occlusion was recanalized completely (TIMI 3). Adjunctive thrombolytics (n = 8, urokinase, 100,000-300,000 U) and/or GP IIb/IIIa antagonist (n = 7, tirofiban, 0.5-1 mg) were administered intra-arterially, and the degree of recanalization further improved in 4 embolic occlusions (TIMI 3). Acute in-stent thrombosis occurred in 2 patients, who received only urokinase without GP IIb/IIIa antagonist. Both of the reoccluded arteries were reopened, by stent recapture in 1 and by intra-arterial administration of GP IIb/IIIa antagonist in the other. Recapture was attempted in 7 cases, of which there were 3 successful outcomes. There was 1 asymptomatic hemorrhagic conversion at the infarction site. The mean improvement of the NIHSS score between baseline and discharge was 12.3 (range, 3-22).
Conclusions: Preliminary results of this study suggest that a self-expanding stent may be safe and efficient for recanalization of acute embolic or dissecting intracranial artery occlusion.
Figures
References
-
- Levy EI, Ecker RD, Horowitz MB, et al. . Stent-assisted intracranial recanalization for acute stroke: early results. Neurosurgery 2006;58:458–63 - PubMed
-
- Zaidat OO, Wolfe T, Hussain SI, et al. . Interventional acute ischemic stroke therapy with intracranial self-expanding stent. Stroke 2008;39:2392–95 - PubMed
-
- Kelly ME, Furlan AJ, Fiorella D. Recanalization of an acute middle cerebral artery occlusion using a self-expanding, reconstrainable intracranial microstent as a temporary endovascular bypass. Stroke 2008;39:1770–73. Epub 2008 Apr 3 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous