

Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program
- PMID: 19892860
- PMCID: PMC2822971
- DOI: 10.1164/rccm.200906-0896OC
Identification of asthma phenotypes using cluster analysis in the Severe Asthma Research Program
Abstract
Rationale: The Severe Asthma Research Program cohort includes subjects with persistent asthma who have undergone detailed phenotypic characterization. Previous univariate methods compared features of mild, moderate, and severe asthma.
Objectives: To identify novel asthma phenotypes using an unsupervised hierarchical cluster analysis.
Methods: Reduction of the initial 628 variables to 34 core variables was achieved by elimination of redundant data and transformation of categorical variables into ranked ordinal composite variables. Cluster analysis was performed on 726 subjects.
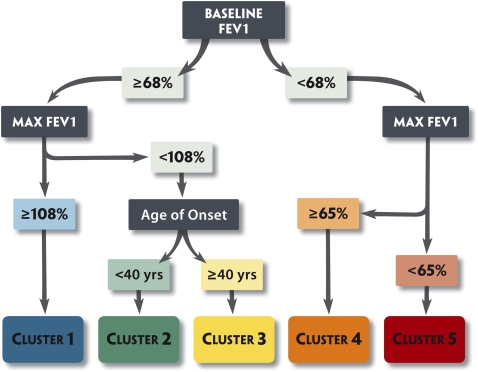
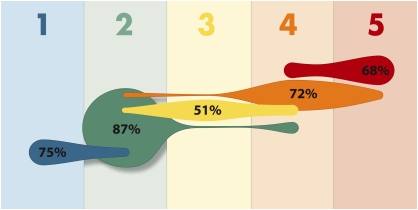
Measurements and main results: Five groups were identified. Subjects in Cluster 1 (n = 110) have early onset atopic asthma with normal lung function treated with two or fewer controller medications (82%) and minimal health care utilization. Cluster 2 (n = 321) consists of subjects with early-onset atopic asthma and preserved lung function but increased medication requirements (29% on three or more medications) and health care utilization. Cluster 3 (n = 59) is a unique group of mostly older obese women with late-onset nonatopic asthma, moderate reductions in FEV(1), and frequent oral corticosteroid use to manage exacerbations. Subjects in Clusters 4 (n = 120) and 5 (n = 116) have severe airflow obstruction with bronchodilator responsiveness but differ in to their ability to attain normal lung function, age of asthma onset, atopic status, and use of oral corticosteroids.
Conclusions: Five distinct clinical phenotypes of asthma have been identified using unsupervised hierarchical cluster analysis. All clusters contain subjects who meet the American Thoracic Society definition of severe asthma, which supports clinical heterogeneity in asthma and the need for new approaches for the classification of disease severity in asthma.
Figures
Comment in
-
Identifying clinical phenotypes of asthma: steps in the right direction.Am J Respir Crit Care Med. 2010 Feb 15;181(4):296-7. doi: 10.1164/rccm.200911-1702ED. Am J Respir Crit Care Med. 2010. PMID: 20130143 No abstract available.
References
-
- National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Bethesda, MD: National Institutes of Health; National Heart, Lung, and Blood Institute; 2007. Publication no. 07-4051 [accessed June 8, 2009]. Available from: http://www.nhlbi.nih.gov/guidelines/asthma
-
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention (GINA). National Institutes of Health; National Heart, Lung, and Blood Institute [accessed June 8, 2009; updated 2008]. Available at http://www.ginasthma.org)
-
- Miller MK, Johnson C, Miller DP, Deniz Y, Bleecker ER, Wenzel SE for the TENOR Study Group. Severity assessment in asthma: an evolving concept. J Allergy Clin Immunol 2005;116:990–995. - PubMed
-
- Wenzel SE. Asthma: defining of the persistent adult phenotypes. Lancet 2006;368:804–813. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL69174/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- HL69116/HL/NHLBI NIH HHS/United States
- M01 RR018390/RR/NCRR NIH HHS/United States
- HL69349/HL/NHLBI NIH HHS/United States
- M01RR07122/RR/NCRR NIH HHS/United States
- M01 RR03186/RR/NCRR NIH HHS/United States
- HL69130/HL/NHLBI NIH HHS/United States
- HL087665/HL/NHLBI NIH HHS/United States
- R01 HL069167/HL/NHLBI NIH HHS/United States
- HL69170/HL/NHLBI NIH HHS/United States
- HL69149/HL/NHLBI NIH HHS/United States
- HL69167/HL/NHLBI NIH HHS/United States
- HL69155/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
