

Defining the intensity of conditioning regimens: working definitions
- PMID: 19896087
- PMCID: PMC2861656
- DOI: 10.1016/j.bbmt.2009.07.004
Defining the intensity of conditioning regimens: working definitions
Abstract
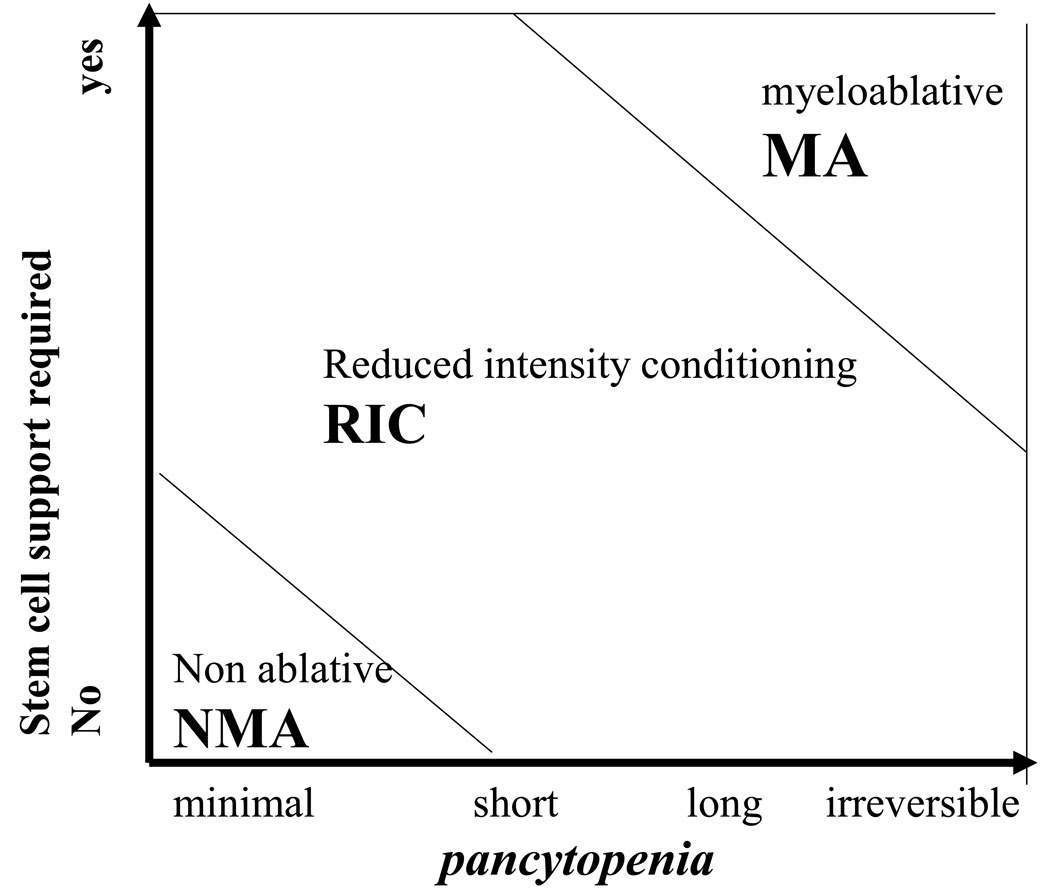
Defining conditioning regimen intensity has become a critical issue for the hemopoietic stem cell transplant (HSCT) community. In the present report we propose to define conditioning regimens in 3 categories: (1) myeloablative (MA) conditioning, (2) reduced-intensity conditioning (RIC), and (3) nonmyeloablative (NMA) conditioning. Assignment to these categories is based on the duration of cytopenia and on the requirement for stem cell (SC) support: MA regimens cause irreversible cytopenia and SC support is mandatory. NMA regimens cause minimal cytopenia, and can be given also without SC support. RIC regimens do not fit criteria for MA or NMA regimens: they cause cytopenia of variable duration, and should be given with stem cell support, although cytopenia may not be irreversible. This report also assigns commonly used regimens to one of these categories, based upon the agents, dose, or combinations. Standardized classification of conditioning regimen intensities will allow comparison across studies and interpretation of study results.
References
-
- Vriesendorp HM. Aims of the conditioning regimen. Exp. Hematol. 2003;31:844–854. - PubMed
-
- Grunebaum E, Mazzolari E, Porta F, Dallera D, Atkinson A, Reid B, Notarangelo LD, Roifman CM. Bone marrow transplantation for severe combined immune deficiency. JAMA. 2006 Feb 1;295(5):508–518. - PubMed
-
- Thomas ED, Buckner CD, Banaji M, Clift RA, Fefer A, Flournoy N, Goodell BW, Hickman RO, Lerner KG, Neiman PE, Sale GE, Sanders JE, Singer J, Stevens M, Storb R, Weiden PL. One hundred patients with acute leukemia treated by chemotherapy, total body irradiation, and allogeneic marrow transplantation. Blood. 1977 Apr;49(4):511–533. - PubMed
-
- Santos GW, Tutschka PJ, Brookmeyer R, Saral R, Beschorner WE, Bias WB, Braine HG, Burns WH, Elfenbein GJ, Kaizer H, et al. Marrow transplantation for acute nonlymphocytic leukemia after treatment with busulfan and cyclophosphamide. N Engl J Med. 1983 Dec 1;309(22):1347–1353. - PubMed
-
- Hobbs JR, Barrett AJ, Chambers D, James DCO, Hugh-Jones K, Byrom N, Henry -K, Lucas CF. Reversal of clinical features of hurler’s disease and biochemical improvement after treatment by bone marrow transplantation. Lancet. 1981;3:709–712. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
