

Efficacy of bipolar radiofrequency endometrial ablation vs thermal balloon ablation for management of menorrhagia: A population-based cohort
- PMID: 19896595
- PMCID: PMC3770134
- DOI: 10.1016/j.jmig.2009.06.022
Efficacy of bipolar radiofrequency endometrial ablation vs thermal balloon ablation for management of menorrhagia: A population-based cohort
Abstract
Study objective: To compare the efficacy of bipolar radiofrequency ablation (RFA) and thermal balloon ablation (TBA) using treatment failure and postprocedure amenorrhea as outcome measures.
Design: Population-based cohort study (Canadian Task Force classification II-2).
Setting: Two medical centers in the upper Midwest.
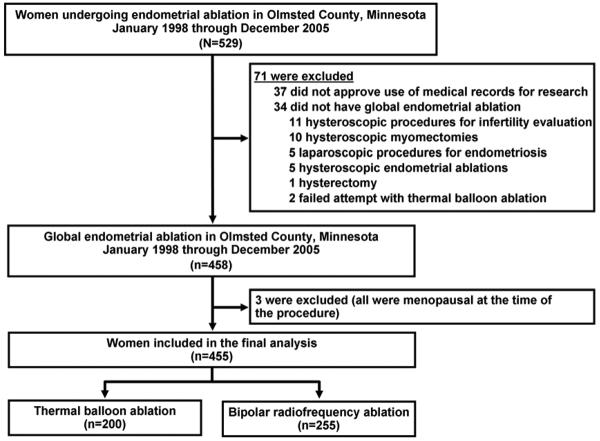
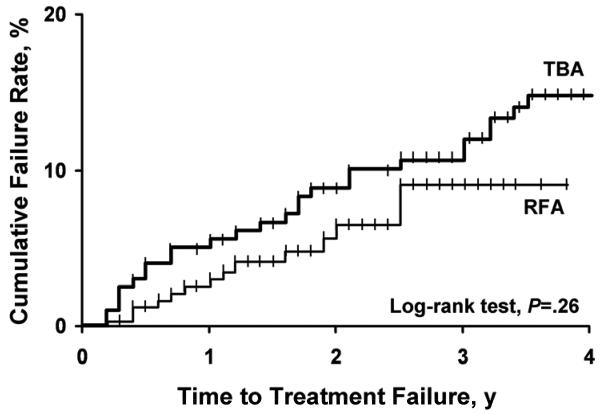
Patients: Using the medical records linkage system of the Rochester Epidemiology Project, we identified 455 residents of Olmsted County, Minnesota, who underwent global endometrial ablation because of menorrhagia from January 1, 1998, through December 31, 2005. Amenorrhea was defined as complete cessation of menstruation that started immediately after ablation and lasted at least 12 months. Treatment failure was defined as necessity of repeat ablation or hysterectomy because of persistent bleeding or pain. Time to treatment failure for each procedure was compared using Kaplan-Meier plots. Relevant clinical data and complications were abstracted from medical records. Risk adjustments were performed using Cox and logistic regression models.
Interventions: Radiofrequency ablation (n=255) and thermal balloon ablation (n=200).
Measurements and main results: Mean (SD) patient age was 43.3 (5.5) years, and median follow-up was 2.2 years. The 3-year cumulative failure rate was 9% (95% confidence interval [CI], 5%-16%) for RFA and 12% (95% CI, 7%-16%) for TBA (p=.26). The difference remained nonsignificant after adjusting for known predictors of treatment failure such as age, parity, pretreatment dysmenorrhea, and tubal ligation (adjusted HR, 0.7; 95% CI, 0.4-1.4; p=.31). However, women had significantly higher rates of amenorrhea after RFA compared with TBA (32% vs 14%; p <.001). This difference remained significant after adjusting for known predictors of amenorrhea such as age, uterine length, and endometrial thickness (adjusted odds ratio, 2.9; 95% CI, 1.7-4.8; p <.001). Complications were infrequent and similar in the 2 groups.
Conclusion: Both RFA and TBA were equally effective treatments for menorrhagia in a population-based cohort. However, women who underwent RFA were 3 times more likely to have postprocedure amenorrhea.
Figures
Comment in
-
Letter to the editor.J Minim Invasive Gynecol. 2010 May-Jun;17(3):401; author reply 401-2. doi: 10.1016/j.jmig.2009.12.009. J Minim Invasive Gynecol. 2010. PMID: 20417438 No abstract available.
-
Letter to the editor.J Minim Invasive Gynecol. 2010 May-Jun;17(3):403; author reply 403-4. doi: 10.1016/j.jmig.2010.01.004. J Minim Invasive Gynecol. 2010. PMID: 20417440 No abstract available.
References
-
- Hallberg L, Hogdahl AM, Nilsson L, Rybo G. Menstrual blood loss: a population study: variation at different ages and attempts to define normality. Acta Obstet Gynecol Scand. 1966;45(3):320–51. - PubMed
-
- Cole SK, Billewicz WZ, Thomson AM. Sources of variation in menstrual blood loss. J Obstet Gynaecol Br Commonw. 1971 Oct;78(10):933–9. - PubMed
-
- Van Eijkeren MA, Christiaens GC, Sixma JJ, Haspels AA. Menorrhagia: a review. Obstet Gynecol Surv. 1989 Jun;44(6):421–9. - PubMed
-
- Warner PE, Critchley HO, Lumsden MA, Campbell-Brown M, Douglas A, Murray GD. Menorrhagia II: is the 80-mL blood loss criterion useful in management of complaint of menorrhagia? Am J Obstet Gynecol. 2004 May;190(5):1224–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
