

Temporal trends in the use of invasive cardiac procedures for non-ST segment elevation acute coronary syndromes according to initial risk stratification
- PMID: 19898699
- PMCID: PMC2776566
- DOI: 10.1016/s0828-282x(09)70163-1
Temporal trends in the use of invasive cardiac procedures for non-ST segment elevation acute coronary syndromes according to initial risk stratification
Abstract
Background: Current guidelines support an early invasive strategy in the management of high-risk non-ST elevation acute coronary syndromes (NSTE-ACS). Although studies in the 1990s suggested that highrisk patients received less aggressive treatment, there are limited data on the contemporary management patterns of NSTE-ACS in Canada.
Objective: To examine the in-hospital use of coronary angiography and revascularization in relation to risk among less selected patients with NSTE-ACS.
Methods: Data from the prospective, multicentre Global Registry of Acute Coronary Events (main GRACE and expanded GRACE2) were used. Between June 1999 and September 2007, 7131 patients from across Canada with a final diagnosis of NSTE-ACS were included the study. The study population was stratified into low-, intermediate- and high-risk groups, based on their calculated GRACE risk score (a validated predictor of in-hospital mortality) and according to time of enrollment.
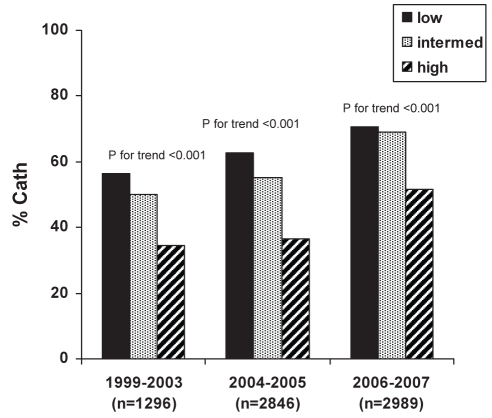
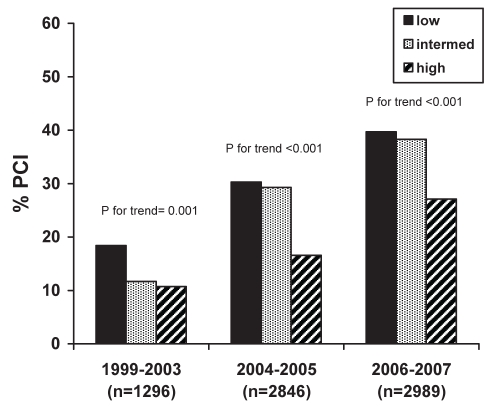
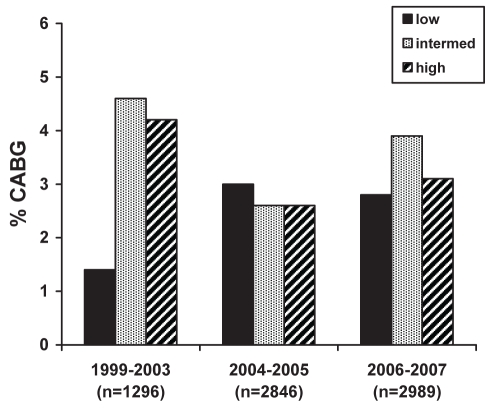
Results: While rates of in-hospital death and reinfarction were significantly (P<0.001) greater in higher-risk patients, the in-hospital use of cardiac catheterization in low- (64.7%), intermediate- (60.3%) and highrisk (42.3%) patients showed an inverse relationship (P<0.001). This trend persisted despite the increase in the overall rates of cardiac catheterization over time (47.9% in 1999 to 2003 versus 51.6% in 2004 to 2005 versus 63.8% in 2006 to 2007; P<0.001). After adjusting for confounders, intermediate-risk (adjusted OR 0.80 [95% CI 0.70 to 0.92], P=0.002) and high-risk (adjusted OR 0.38 [95% CI 0.29 to 0.48], P<0.001) patients remained less likely to undergo in-hospital cardiac catheterization.
Conclusion: Despite the temporal increase in the use of invasive cardiac procedures, they remain paradoxically targeted toward low-risk patients with NSTE-ACS in contemporary practice. This treatment-risk paradox needs to be further addressed to maximize the benefits of invasive therapies in Canada.
HISTORIQUE :: Les lignes directrices actuelles appuient une stratégie effractive précoce dans la prise en charge des syndromes coronariens aigus sans élévation du segment ST (SCA-SÉST) à haut risque. Même si, dans les années 1990, des études ont laissé supposer que les patients à haut risque recevaient un traitement moins énergique, les données sur la prise en charge courante des profils de SCA-SÉST demeurent limitées au Canada.
OBJECTIF :: Examiner l’utilisation de la coronarographie et de la revascularisation en milieu hospitalier par rapport au risque chez des patients moins sélectionnés ayant une SCA-SÉST.
MÉTHODOLOGIE :: Les auteurs ont utilisé les données de l’étude prospective multicentrique sur le registre mondial des événements coronariens aigus (étude GRACE principale et GRACE élargie2). Entre juin 1999 et septembre 2007, 7 131 patients de partout au Canada ayant un diagnostic définitif de SCA-SÉST ont participé à l’étude. Cette population était stratifiée en groupes à faible risque, à risque moyen et à haut risque, d’après l’indice de risque calculé pour l’étude GRACE (un prédicteur validé de la mortalité en milieu hospitalier) et le moment de leur inscription à l’étude.
RÉSULTATS :: Les taux de décès et de nouvel infarctus en milieu hospitalier étaient considérablement plus élevés (P<0,001) chez les patients à plus haut risque, mais l’utilisation du cathétérisme cardiaque en milieu hospitalier était inversement proportionnelle (P<0,001) chez les patients à faible risque (64,7 %), à risque moyen (60,3 %) et à haut risque (42,3 %). Cette tendance a persisté malgré l’augmentation des taux globaux de cathétérisme cardiaque au fil du temps (47,9 % de 1999 à 2003, par rapport à 51,6 % en 2004 et 2005 et à 63,8 % en 2006 et 2007; P<0,001). Après rajustement compte tenu des variables confusionnelles, les patients à risque moyen (RRR 0,80 [95% IC 0,70 à 0,92], P=0,002) et à haut risque (RRR 0,38 [95% IC 0,29 à 0,48], P<0,001) demeuraient moins susceptibles de subir un cathétérisme cardiaque en milieu hospitalier.
CONCLUSION :: Malgré l’augmentation temporelle de l’utilisation des interventions cardiaques effractives, dans la pratique actuelle, ces interventions demeurent paradoxalement ciblées vers les patients à faible risque ayant un SCA-SÉST. Il faut étudier davantage ce paradoxe entre le traitement et le risque pour maximiser les bienfaits des thérapies effractives au Canada.
Figures
References
-
- Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction – summary article: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2002;40:1366–74. - PubMed
-
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2007;50:e1–57. - PubMed
-
- Bhatt DL, Roe MT, Peterson ED, et al. Utilization of early invasive management strategies for high-risk patients with non-ST-segment elevation acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative. JAMA. 2004;292:2096–104. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
