

Plasma concentrations of inflammatory cytokines rise rapidly during ECMO-related SIRS due to the release of preformed stores in the intestine
- PMID: 19901912
- PMCID: PMC2799549
- DOI: 10.1038/labinvest.2009.119
Plasma concentrations of inflammatory cytokines rise rapidly during ECMO-related SIRS due to the release of preformed stores in the intestine
Abstract
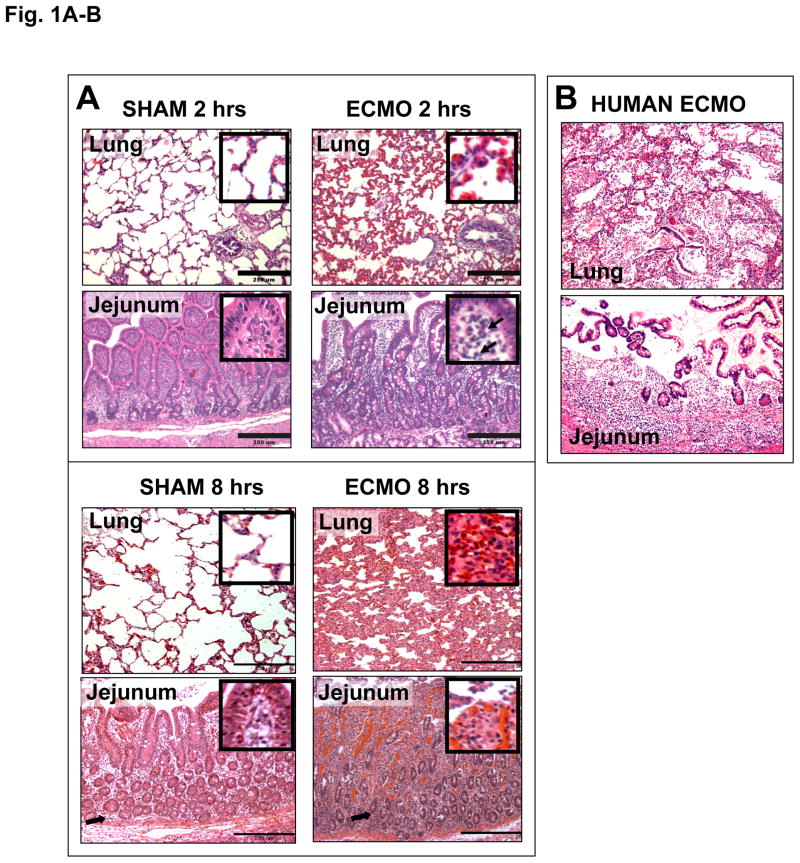
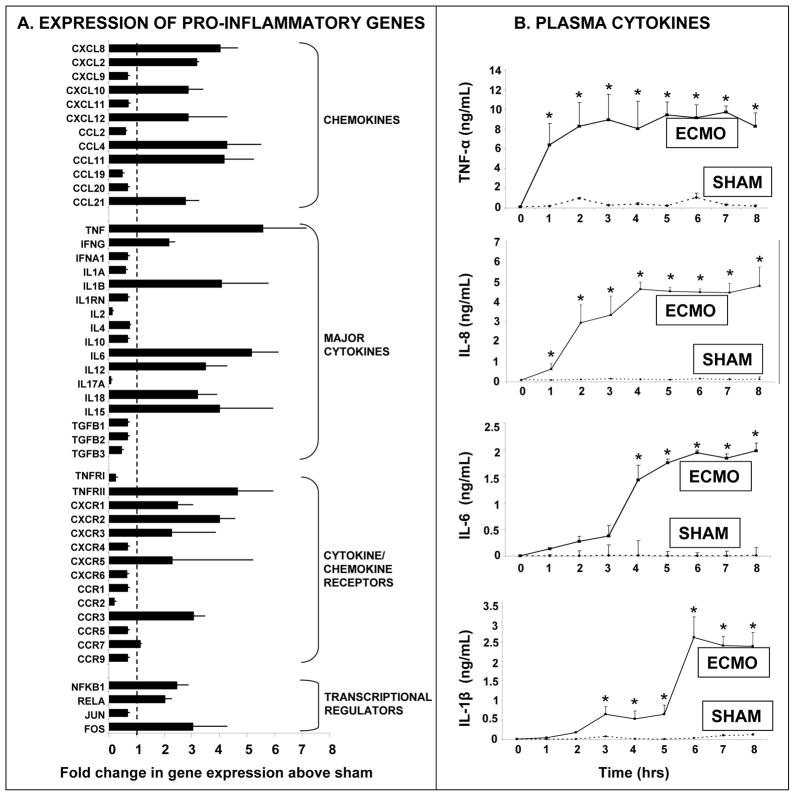
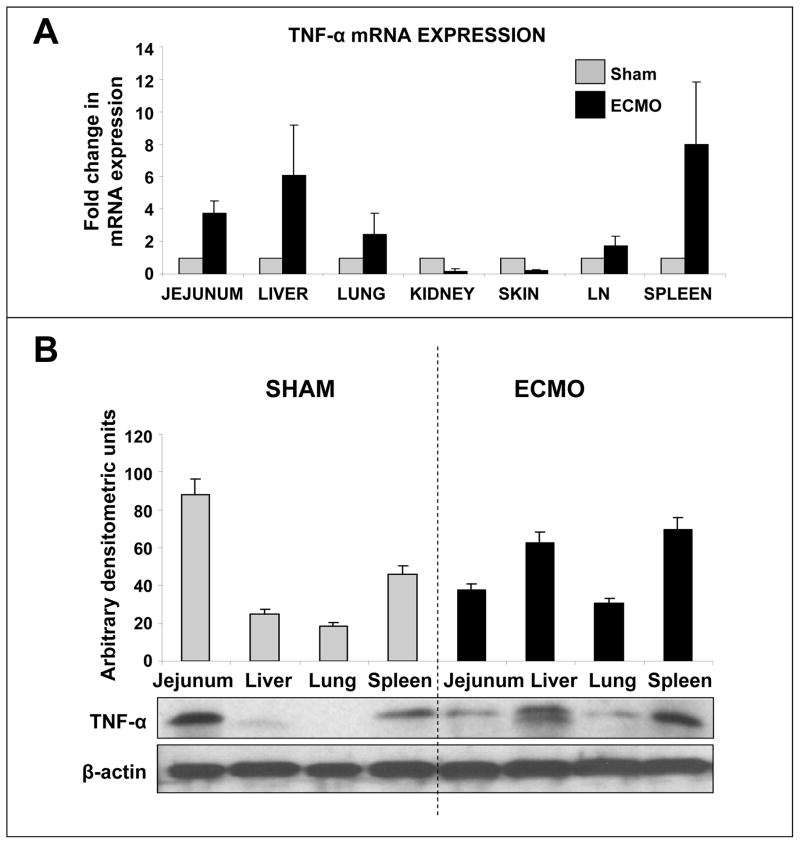
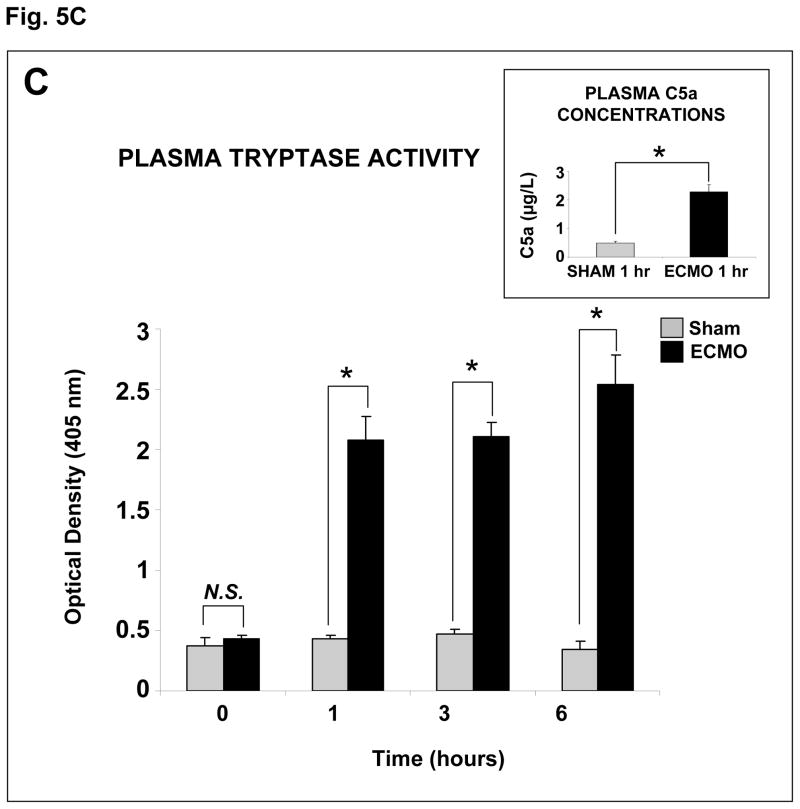
Extracorporeal membrane oxygenation (ECMO) is a life-saving support system used in neonates and young children with severe cardiorespiratory failure. Although ECMO has reduced mortality in these critically ill patients, almost all patients treated with ECMO develop a systemic inflammatory response syndrome (SIRS) characterized by a 'cytokine storm', leukocyte activation, and multisystem organ dysfunction. We used a neonatal porcine model of ECMO to investigate whether rising plasma concentrations of inflammatory cytokines during ECMO reflect de novo synthesis of these mediators in inflamed tissues, and therefore, can be used to assess the severity of ECMO-related SIRS. Previously healthy piglets (3-week-old) were subjected to venoarterial ECMO for up to 8 h. SIRS was assessed by histopathological analysis, measurement of neutrophil activation (flow cytometry), plasma cytokine concentrations (enzyme immunoassays), and tissue expression of inflammatory genes (PCR/western blots). Mast cell degranulation was investigated by measurement of plasma tryptase activity. Porcine neonatal ECMO was associated with systemic inflammatory changes similar to those seen in human neonates. Tumor necrosis factor-alpha (TNF-alpha) and interleukin-8 (IL-8) concentrations rose rapidly during the first 2 h of ECMO, faster than the tissue expression of these cytokines. ECMO was associated with increased plasma mast cell tryptase activity, indicating that increased plasma concentrations of inflammatory cytokines during ECMO may result from mast cell degranulation and associated release of preformed cytokines stored in mast cells. TNF-alpha and IL-8 concentrations rose faster in plasma than in the peripheral tissues during ECMO, indicating that rising plasma levels of these cytokines immediately after the initiation of ECMO may not reflect increasing tissue synthesis of these cytokines. Mobilization of preformed cellular stores of inflammatory cytokines such as in mucosal mast cells may have an important pathophysiological role in ECMO-related SIRS.
Conflict of interest statement
Figures



Similar articles
-
Intestinal epithelial apoptosis initiates gut mucosal injury during extracorporeal membrane oxygenation in the newborn piglet.Lab Invest. 2014 Feb;94(2):150-60. doi: 10.1038/labinvest.2013.149. Epub 2013 Dec 23. Lab Invest. 2014. PMID: 24365747 Free PMC article.
-
Extracorporeal membrane oxygenation causes loss of intestinal epithelial barrier in the newborn piglet.Pediatr Res. 2010 Aug;68(2):128-33. doi: 10.1203/PDR.0b013e3181e4c9f8. Pediatr Res. 2010. PMID: 20442689 Free PMC article.
-
Effects of continuous renal replacement therapy on intestinal mucosal barrier function during extracorporeal membrane oxygenation in a porcine model.J Cardiothorac Surg. 2014 Apr 23;9:72. doi: 10.1186/1749-8090-9-72. J Cardiothorac Surg. 2014. PMID: 24758270 Free PMC article.
-
Systemic inflammatory response to exhaustive exercise. Cytokine kinetics.Exerc Immunol Rev. 2002;8:6-48. Exerc Immunol Rev. 2002. PMID: 12690937 Review.
-
The inflammatory response to extracorporeal membrane oxygenation (ECMO): a review of the pathophysiology.Crit Care. 2016 Nov 28;20(1):387. doi: 10.1186/s13054-016-1570-4. Crit Care. 2016. PMID: 27890016 Free PMC article. Review.
Cited by
-
Longitudinal Cytokine Profiling in Patients with Severe COVID-19 on Extracorporeal Membrane Oxygenation and Hemoadsorption.Am J Respir Crit Care Med. 2021 Jun 1;203(11):1433-1435. doi: 10.1164/rccm.202011-4140LE. Am J Respir Crit Care Med. 2021. PMID: 33725469 Free PMC article. No abstract available.
-
Differential effects of octanoate and heptanoate on myocardial metabolism during extracorporeal membrane oxygenation in an infant swine model.Am J Physiol Heart Circ Physiol. 2015 Oct;309(7):H1157-65. doi: 10.1152/ajpheart.00298.2015. Epub 2015 Jul 31. Am J Physiol Heart Circ Physiol. 2015. PMID: 26232235 Free PMC article.
-
Inflammation and Oxidative Stress in the Context of Extracorporeal Cardiac and Pulmonary Support.Front Immunol. 2022 Mar 4;13:831930. doi: 10.3389/fimmu.2022.831930. eCollection 2022. Front Immunol. 2022. PMID: 35309362 Free PMC article. Review.
-
Intraoperative vasoplegic syndrome in patients with fulminant myocarditis on ventricular assist device placement.J Anesth. 2019 Apr;33(2):304-310. doi: 10.1007/s00540-019-02625-5. Epub 2019 Mar 12. J Anesth. 2019. PMID: 30863956
-
Current Understanding of Leukocyte Phenotypic and Functional Modulation During Extracorporeal Membrane Oxygenation: A Narrative Review.Front Immunol. 2021 Jan 8;11:600684. doi: 10.3389/fimmu.2020.600684. eCollection 2020. Front Immunol. 2021. PMID: 33488595 Free PMC article. Review.
References
-
- Kelly RE, Jr, Phillips JD, Foglia RP, Bjerke HS, Barcliff LT, Petrus L, et al. Pulmonary edema and fluid mobilization as determinants of the duration of ECMO support. J Pediatr Surg. 1991;26(9):1016–1022. - PubMed
-
- Ford JW. Neonatal ECMO: Current controversies and trends. Neonatal Netw. 2006;25(4):229–238. - PubMed
-
- Khoshbin E, Dux AE, Killer H, Sosnowski AW, Firmin RK, Peek GJ. A comparison of radiographic signs of pulmonary inflammation during ECMO between silicon and poly-methyl pentene oxygenators. Perfusion. 2007;22(1):15–21. - PubMed
-
- Butler J, Pathi VL, Paton RD, Logan RW, MacArthur KJ, Jamieson MP, et al. Acute-phase responses to cardiopulmonary bypass in children weighing less than 10 kilograms. Ann Thorac Surg. 1996;62(2):538–542. - PubMed
-
- Kozik DJ, Tweddell JS. Characterizing the inflammatory response to cardiopulmonary bypass in children. Ann Thorac Surg. 2006;81(6):S2347–2354. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
