

Functional recovery following an end to side neurorrhaphy of the accessory nerve to the suprascapular nerve: case report
- PMID: 19902308
- PMCID: PMC2920384
- DOI: 10.1007/s11552-009-9242-3
Functional recovery following an end to side neurorrhaphy of the accessory nerve to the suprascapular nerve: case report
Abstract
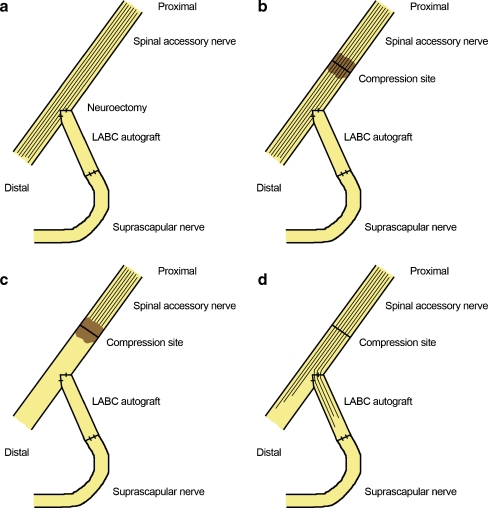
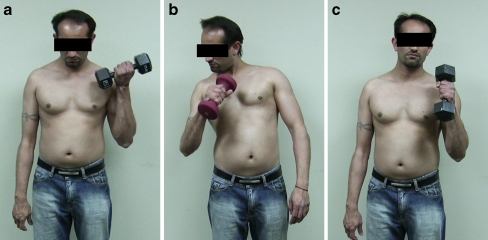
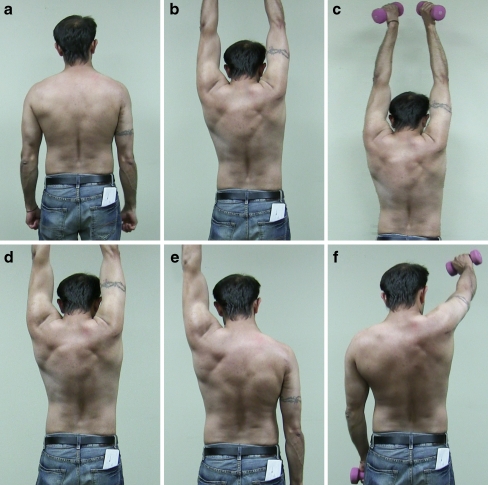
The use of end-to-side neurrorhaphy remains a controversial topic in peripheral nerve surgery. The authors report the long-term functional outcome following a modified end-to-side motor reinnervation using the spinal accessory to innervate the suprascapular nerve following a C5 to C6 avulsion injury. Additionally, functional outcomes of an end-to-end neurotization of the triceps branch to the axillary nerve and double fascicular transfer of the ulnar and medial nerve to the biceps and brachialis are presented. Excellent functional recoveries are found in respect to shoulder abduction and flexion and elbow flexion.
Electronic supplementary material: The online version of this article (doi:10.1007/s11552-009-9242-3) contains supplementary material, which is available to authorized users.
Figures
References
-
- Asaoka K, Sawamura Y. Hypoglossal-facial nerve side-to-end anastomosis. J Neurosurg. 1999;91:163–164. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
