

Effects of baclofen on motor units paralysed by chronic cervical spinal cord injury
- PMID: 19903733
- PMCID: PMC2857957
- DOI: 10.1093/brain/awp285
Effects of baclofen on motor units paralysed by chronic cervical spinal cord injury
Abstract
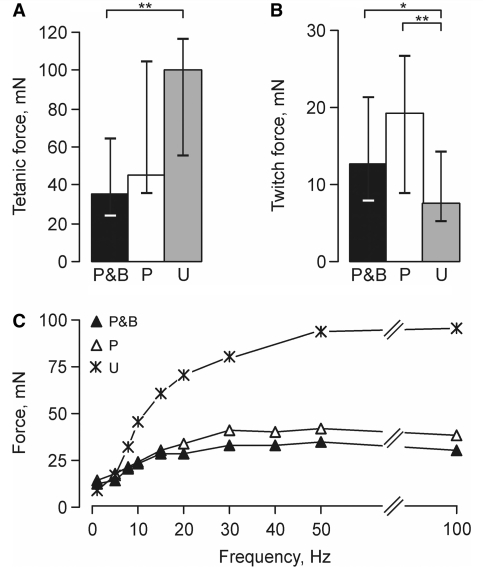
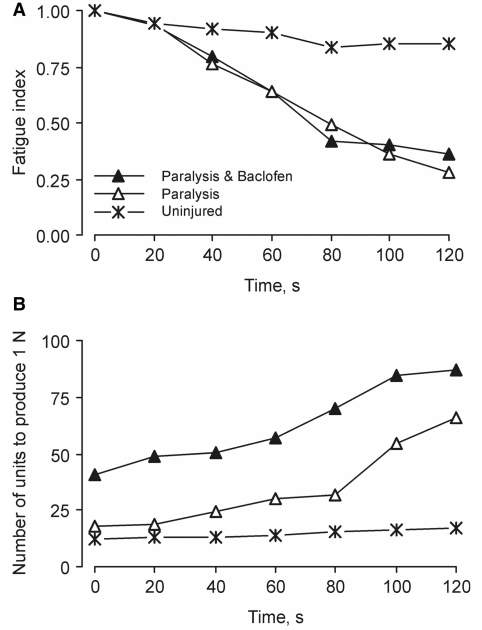
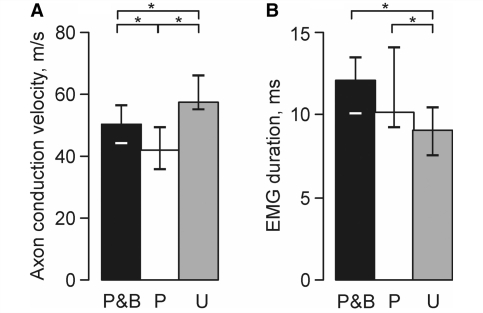
Baclofen, a gamma-aminobutyric acid receptor(B) agonist, is used to reduce symptoms of spasticity (hyperreflexia, increases in muscle tone, involuntary muscle activity), but the long-term effects of sustained baclofen use on skeletal muscle properties are unclear. The aim of our study was to evaluate whether baclofen use and paralysis due to cervical spinal cord injury change the contractile properties of human thenar motor units more than paralysis alone. Evoked electromyographic activity and force were recorded in response to intraneural stimulation of single motor axons to thenar motor units. Data from three groups of motor units were compared: 23 paralysed units from spinal cord injured subjects who take baclofen and have done so for a median of 7 years, 25 paralysed units from spinal cord injured subjects who do not take baclofen (median: 10 years) and 45 units from uninjured control subjects. Paralysed motor unit properties were independent of injury duration and level. With paralysis and baclofen, the median motor unit tetanic forces were significantly weaker, twitch half-relaxation times longer and half maximal forces reached at lower frequencies than for units from uninjured subjects. The median values for these same parameters after paralysis alone were comparable to control data. Axon conduction velocities differed across groups and were slowest for paralysed units from subjects who were not taking baclofen and fastest for units from the uninjured. Greater motor unit weakness with long-term baclofen use and paralysis will make the whole muscle weaker and more fatigable. Significantly more paralysed motor units need to be excited during patterned electrical stimulation to produce any given force over time. The short-term benefits of baclofen on spasticity (e.g. management of muscle spasms that may otherwise hinder movement or social interactions) therefore have to be considered in relation to its possible long-term effects on muscle rehabilitation. Restoring the strength and speed of paralysed muscles to pre-injury levels may require more extensive therapy when baclofen is used chronically.
Figures

References
-
- Adams MM, Hicks AL. Spasticity after spinal cord injury. Spinal Cord. 2005;43:577–86. - PubMed
-
- Alaimo MA, Smith JL, Roy RR, Edgerton VR. EMG activity of slow and fast ankle extensors following spinal cord transection. J Appl Physiol. 1984;56:1608–13. - PubMed
-
- Burke D, Andrews CJ, Knowles L. The action of a GABA derivative in human spasticity. J Neurol Sci. 1971;14:199–208. - PubMed
-
- Carp JS, Wolpaw JR. Motoneuron plasticity underlying operantly conditioned decrease in primate H-reflex. J Neurophysiol. 1994;72:431–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
