

Patterns of use and risks associated with erythropoiesis-stimulating agents among Medicare patients with cancer
- PMID: 19903808
- PMCID: PMC2786918
- DOI: 10.1093/jnci/djp387
Patterns of use and risks associated with erythropoiesis-stimulating agents among Medicare patients with cancer
Erratum in
- J Natl Cancer Inst. 2010 Feb 24;102(4):282-3
Abstract
Background: Erythropoiesis-stimulating agents (erythropoietin and darbepoietin) have been approved to reduce the number of blood transfusions required during chemotherapy; however, concerns about the risks of venous thromboembolism and mortality exist.
Methods: We identified patients who were aged 65 years or older in the Surveillance, Epidemiology, and End Results-Medicare database; who were diagnosed with colon, non-small cell lung, or breast cancer or with diffuse large B-cell lymphoma from January 1, 1991, through December 31, 2002; and who received chemotherapy. The main outcome measures were claims for use of an erythropoiesis-stimulating agent, blood transfusion, venous thromboembolism (ie, deep vein thrombosis or pulmonary embolism), and overall survival. We used multivariable logistic regression models to analyze the association of erythropoiesis-stimulating agent use with clinical and demographic variables. We used time-dependent Cox proportional hazards models to analyze the association of time to receipt of first erythropoiesis-stimulating agent with venous thromboembolism and overall survival. All statistical tests were two-sided.
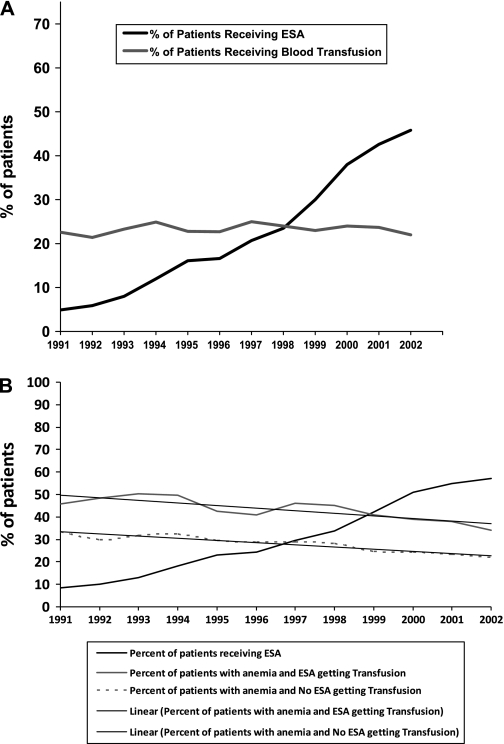
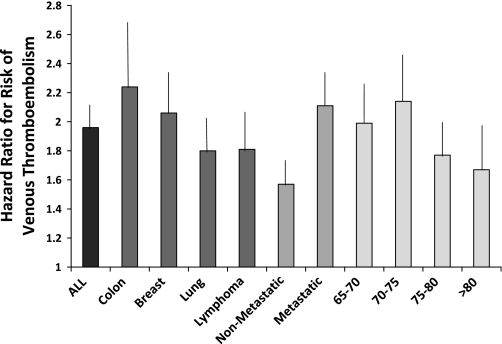
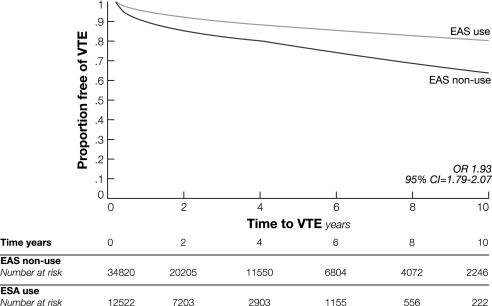
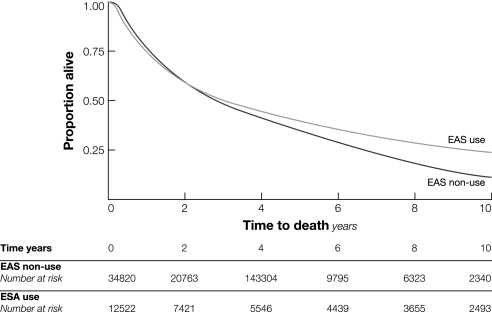
Results: Among 56,210 patients treated with chemotherapy from 1991 through 2002, 15,346 (27%) received an erythropoiesis-stimulating agent. The proportion of patients receiving erythropoiesis-stimulating agents increased from 4.8% in 1991 to 45.9% in 2002 (P < .001). Use was associated with more recent diagnosis, younger age, urban residence, comorbidities, receipt of radiation therapy, female sex, and metastatic or recurrent cancer. The rate of blood transfusion per year during 1991-2002 remained constant at 22%. Venous thromboembolism developed in 1796 (14.3%) of the 12,522 patients who received erythropoiesis-stimulating agent and 3400 (9.8%) of the 34,820 patients who did not (hazard ratio = 1.93, 95% confidence interval = 1.79 to 2.07). Overall survival was similar in both groups.
Conclusion: Use of erythropoiesis-stimulating agent increased rapidly after its approval in 1991, but the blood transfusion rate did not change. Use of erythropoiesis-stimulating agents was associated with an increased risk of venous thromboembolism but not of mortality.
Figures
References
-
- Vansteenkiste J, Pirker R, Massuti B, et al. Double-blind, placebo-controlled, randomized phase III trial of darbepoetin alfa in lung cancer patients receiving chemotherapy. J Natl Cancer Inst. 2002;94(16):1211–1220. - PubMed
-
- Henry DH, Brooks BJ, Jr, Case DC, Jr, et al. Recombinant human erythropoietin therapy for anemic cancer patients receiving cisplatin chemotherapy. Canc J Sci Am. 1995;1(4):252–260. - PubMed
-
- Littlewood TJ, Bajetta E, Nortier JW, Vercammen E, Rapoport B. Effects of epoetin alfa on hematologic parameters and quality of life in cancer patients receiving nonplatinum chemotherapy: results of a randomized, double-blind, placebo-controlled trial. J Clin Oncol. 2001;19(11):2865–2874. - PubMed
-
- Corwin HL, Gettinger A, Fabian TC, et al. Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med. 2007;357(10):965–976. - PubMed
-
- Henke M, Laszig R, Rube C, et al. Erythropoietin to treat head and neck cancer patients with anaemia undergoing radiotherapy: randomised, double-blind, placebo-controlled trial. Lancet. 2003;362(9392):1255–1260. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
