

Overdetection, overtreatment and costs in prostate-specific antigen screening for prostate cancer
- PMID: 19904272
- PMCID: PMC2788248
- DOI: 10.1038/sj.bjc.6605422
Overdetection, overtreatment and costs in prostate-specific antigen screening for prostate cancer
Abstract
Background: Prostate cancer screening with prostate-specific antigen (PSA) has shown to reduce prostate cancer mortality in the European Randomised study of Screening for Prostate Cancer (ERSPC) trial. Overdetection and overtreatment are substantial unfavourable side effects with consequent healthcare costs. In this study the effects of introducing widespread PSA screening is evaluated.
Methods: The MISCAN model was used to simulate prostate cancer growth and detection in a simulated cohort of 100,000 men (European standard population) over 25 years. PSA screening from age 55 to 70 or 75, with 1, 2 and 4-year-intervals is simulated. Number of diagnoses, PSA tests, biopsies, treatments, deaths and corresponding costs for 100,000 men and for United Kingdom and United States are compared.
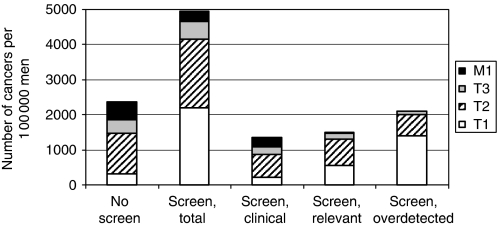
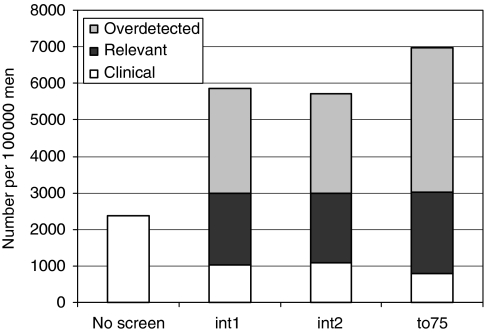
Results: Without screening 2378 men per 100,000 were predicted to be diagnosed with prostate cancer compared with 4956 men after screening at 4-year intervals. By introducing screening, the costs would increase with 100% to 60,695,000 euro. Overdetection is related to 39% of total costs (23,669,000 euro). Screening until age 75 is relatively most expensive because of the costs of overtreatment.
Conclusion: Introduction of PSA screening will increase total healthcare costs for prostate cancer substantially, of which the actual screening costs will be a small part.
Figures
References
-
- Beemsterboer PM, de Koning HJ, Birnie E, van der Maas PJ, Schroder FH (1999) Advanced prostate cancer: course, care, and cost implications. Prostate 40: 97–104 - PubMed
-
- Burkhardt JH, Litwin MS, Rose CM, Correa RJ, Sunshine JH, Hogan C, Hayman JA (2002) Comparing the costs of radiation therapy and radical prostatectomy for the initial treatment of early-stage prostate cancer. J Clin Oncol 20: 2869–2875 - PubMed
-
- Chelladurai AJ, Gunendran T, Nicholson C, Matanhelia SS, Blades RA (2008) The economic and workload impact of ‘backdoor’ prostate-specific antigen screening on the UK National Health Service: a single-centre experience. BJU Int 101: 289–292 - PubMed
-
- Crawford ED, Abrahamsson PA (2008) PSA-based screening for prostate cancer: how does it compare with other cancer screening tests? Eur Urol 54: 262–273 - PubMed
-
- Dong F, Kattan MW, Steyerberg EW, Jones JS, Stephenson AJ, Schroder FH, Klein EA (2008) Validation of pretreatment nomograms for predicting indolent prostate cancer: efficacy in contemporary urological practice. J Urol 180: 150–154 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
