

Hyperparasitaemia and low dosing are an important source of anti-malarial drug resistance
- PMID: 19906307
- PMCID: PMC2784792
- DOI: 10.1186/1475-2875-8-253
Hyperparasitaemia and low dosing are an important source of anti-malarial drug resistance
Abstract
Background: Preventing the emergence of anti-malarial drug resistance is critical for the success of current malaria elimination efforts. Prevention strategies have focused predominantly on qualitative factors, such as choice of drugs, use of combinations and deployment of multiple first-line treatments. The importance of anti-malarial treatment dosing has been underappreciated. Treatment recommendations are often for the lowest doses that produce "satisfactory" results.
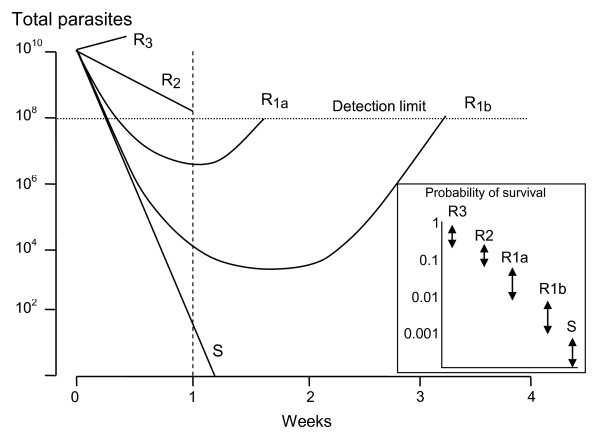
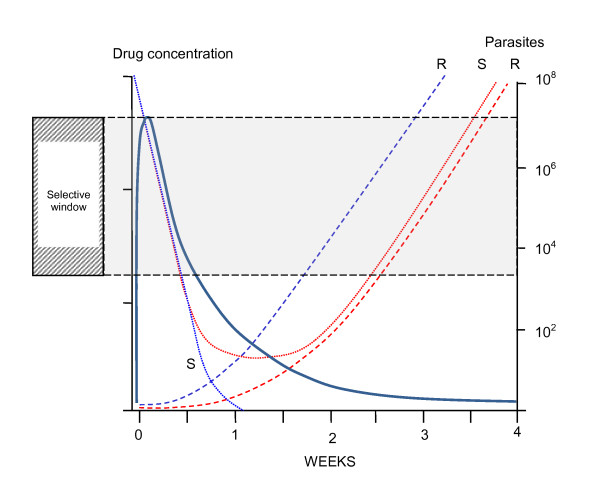
Methods: The probability of de-novo resistant malaria parasites surviving and transmitting depends on the relationship between their degree of resistance and the blood concentration profiles of the anti-malarial drug to which they are exposed. The conditions required for the in-vivo selection of de-novo emergent resistant malaria parasites were examined and relative probabilities assessed.
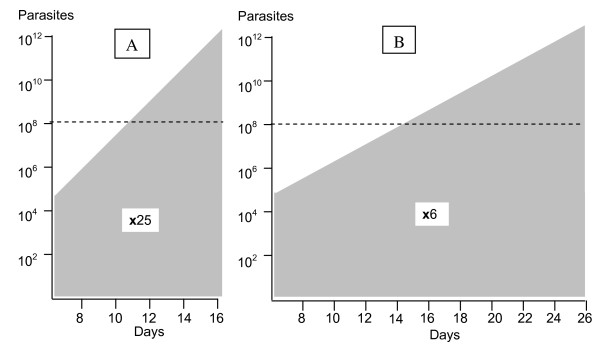
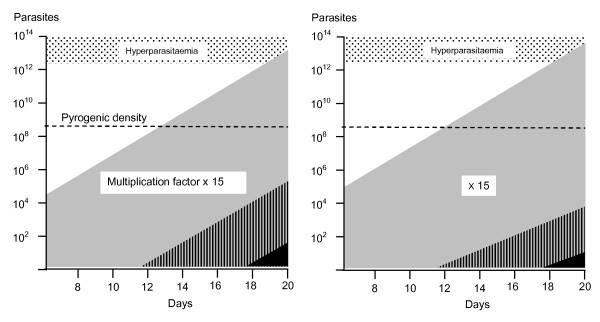
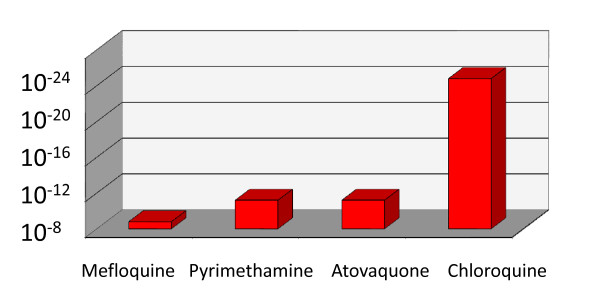
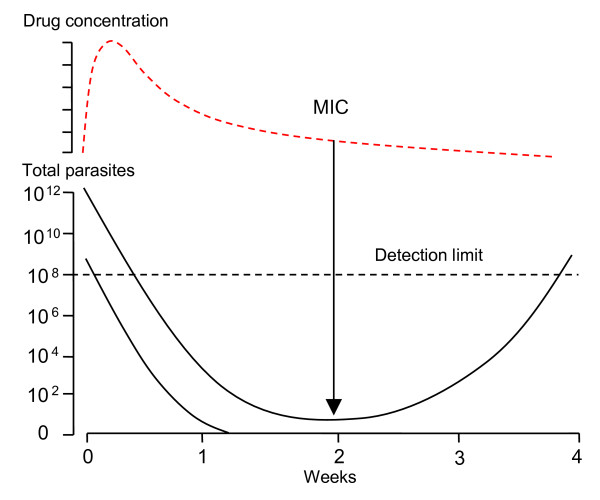
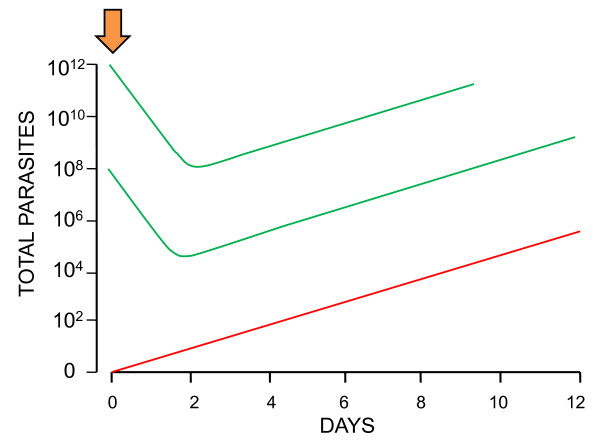
Results: Recrudescence is essential for the transmission of de-novo resistance. For rapidly eliminated anti-malarials high-grade resistance can arise from a single drug exposure, but low-grade resistance can arise only from repeated inadequate treatments. Resistance to artemisinins is, therefore, unlikely to emerge with single drug exposures. Hyperparasitaemic patients are an important source of de-novo anti-malarial drug resistance. Their parasite populations are larger, their control of the infection insufficient, and their rates of recrudescence following anti-malarial treatment are high. As use of substandard drugs, poor adherence, unusual pharmacokinetics, and inadequate immune responses are host characteristics, likely to pertain to each recurrence of infection, a small subgroup of patients provides the particular circumstances conducive to de-novo resistance selection and transmission.
Conclusion: Current dosing recommendations provide a resistance selection opportunity in those patients with low drug levels and high parasite burdens (often children or pregnant women). Patients with hyperparasitaemia who receive outpatient treatments provide the greatest risk of selecting de-novo resistant parasites. This emphasizes the importance of ensuring that only quality-assured anti-malarial combinations are used, that treatment doses are optimized on the basis of pharmacodynamic and pharmacokinetic assessments in the target populations, and that patients with heavy parasite burdens are identified and receive sufficient treatment to prevent recrudescence.
Figures
References
-
- Peters W. Chemotherapy and drug resistance in malaria. 2. Academic press, London; 1987.
-
- Peters W. The prevention of antimalarial drug resistance. Pharmacol Ther. 1990;47:499–508. - PubMed
-
- Barnes KI, White NJ. Population biology and antimalarial resistance: The transmission of antimalarial drug resistance in Plasmodium falciparum. Acta Trop. 2005;94:230–224. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
