

Evaluation of modernisation of adult critical care services in England: time series and cost effectiveness analysis
- PMID: 19906740
- PMCID: PMC2776132
- DOI: 10.1136/bmj.b4353
Evaluation of modernisation of adult critical care services in England: time series and cost effectiveness analysis
Abstract
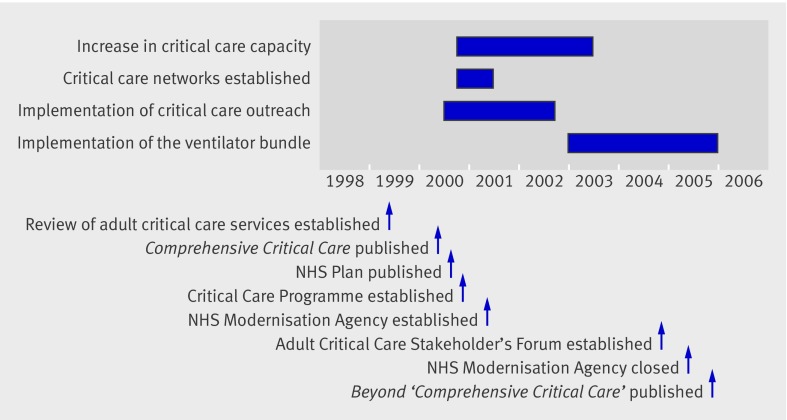
Objective: To evaluate the impact and cost effectiveness of a programme to transform adult critical care throughout England initiated in late 2000.
Design: Evaluation of trends in inputs, processes, and outcomes during 1998-2000 compared with last quarter of 2000-6.
Setting: 96 critical care units in England.
Participants: 349,817 admissions to critical care units.
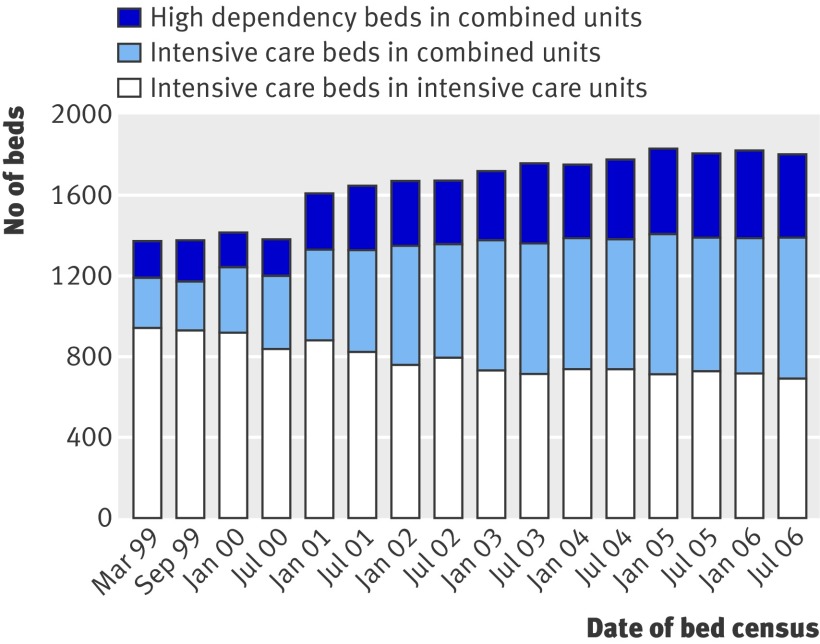
Interventions: Adoption of key elements of modernisation and increases in capacity. Units were categorised according to when they adopted key elements of modernisation and increases in capacity.
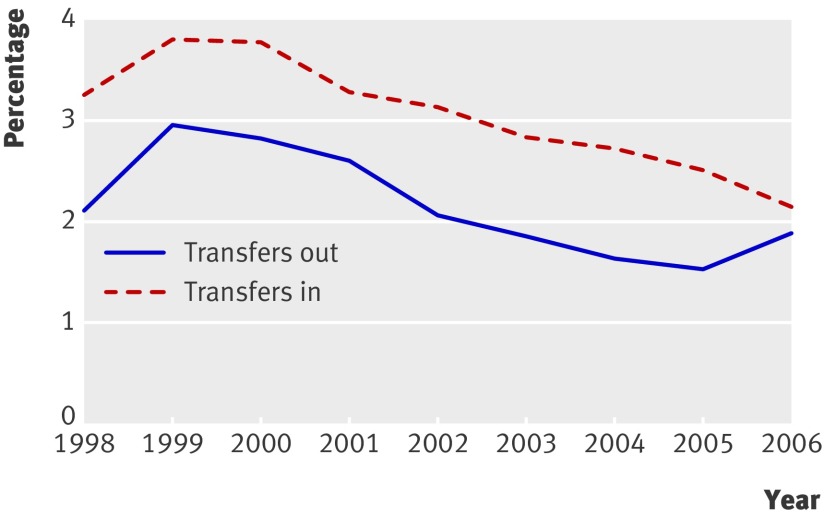
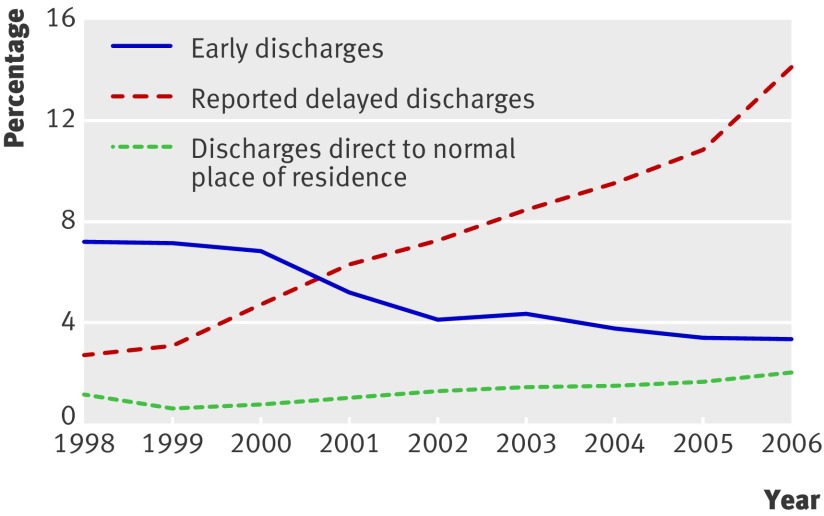
Main outcome measures: Trends in inputs (beds, costs), processes (transfers between units, discharge practices, length of stay, readmissions), and outcomes (unit and hospital mortality), with adjustment for case mix. Differences in annual costs and quality adjusted life years (QALYs) adjusted for case mix were used to calculate net monetary benefits (valuing a QALY gain at pound20,000 ($33,170, euro22 100)). The incremental net monetary benefits were reported as the difference in net monetary benefits after versus before 2000.
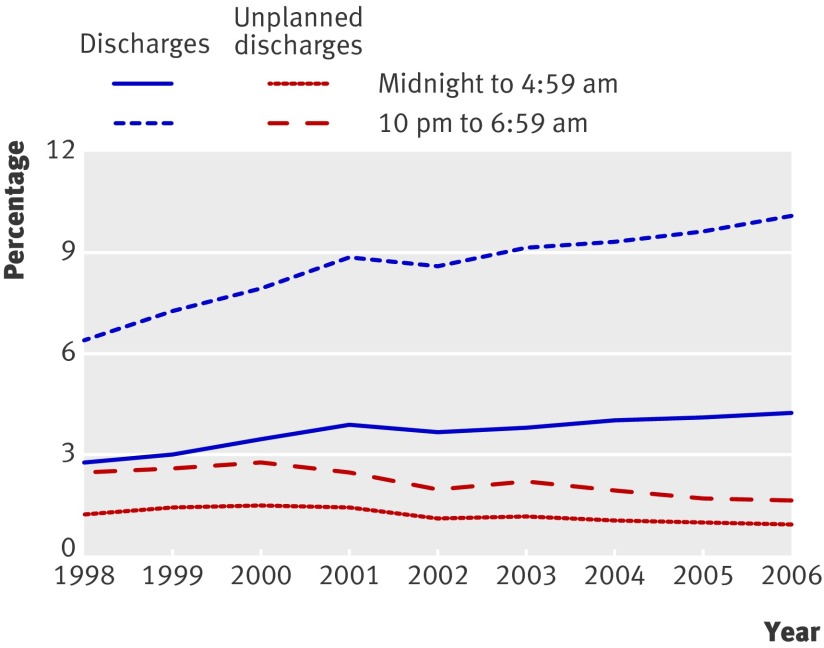
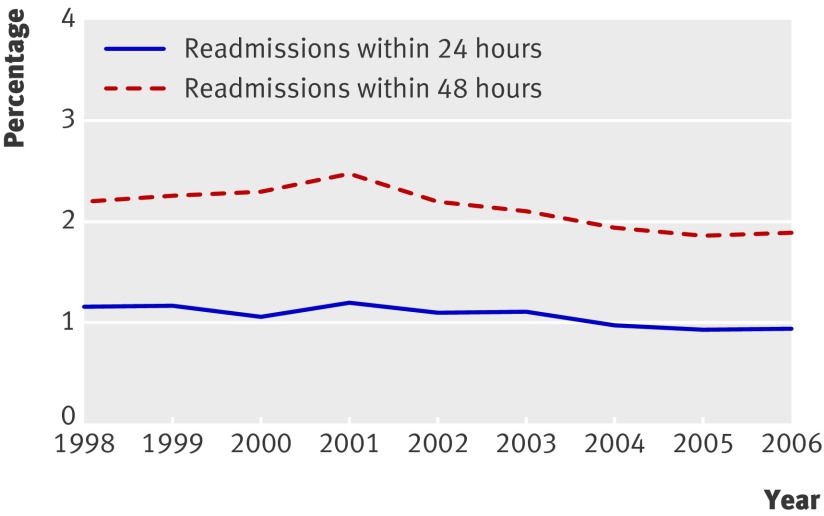
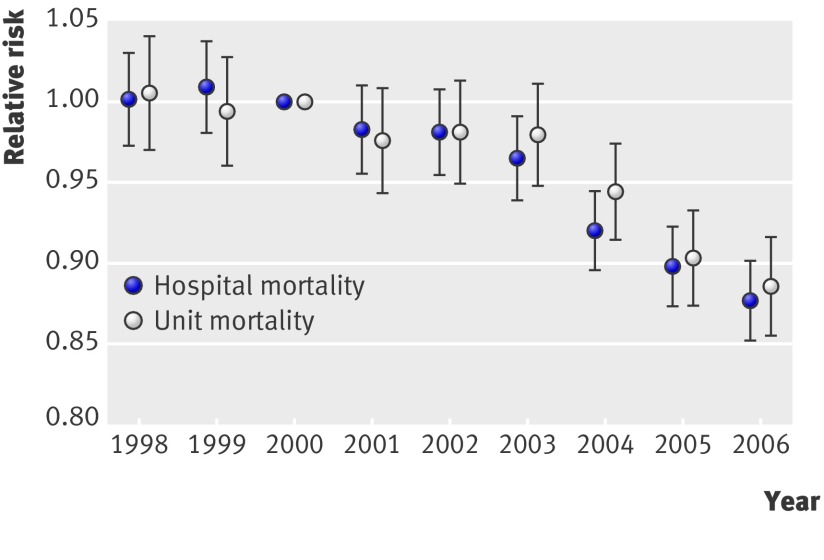
Results: In the six years after 2000, the risk of unit mortality adjusted for case mix fell by 11.3% and hospital mortality by 13.4% compared with the steady state in the three preceding years. This was accompanied by substantial reductions both in transfers between units and in unplanned night discharges. The mean annual net monetary benefit increased significantly after 2000 (from pound402 ($667, euro445) to pound1096 ($1810, euro1210)), indicating that the changes were relatively cost effective. The relative contribution of the different initiatives to these improvements is unclear.
Conclusion: Substantial improvements in NHS critical care have occurred in England since 2000. While it is unclear which factors were responsible, collectively the interventions represented a highly cost effective use of NHS resources.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Department of Health. Comprehensive critical care: a review of adult critical care services. DH, 2000.
-
- Department of Health. The NHS plan. DH, 2000.
-
- NHS Modernisation Agency. 10 high impact changes for service improvement and delivery: a guide for NHS leaders. NHS Modernisation Agency, 2004.
-
- Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. J Comm J Qual Patient Saf 2005;31:243-8. - PubMed
-
- Robson W. The saving lives and 100,000 lives programmes: good news for critical care nurses. Intensive Crit Care Nurs 2006;22:1-3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical