

CYP3A4 and CYP3A5 polymorphisms and blood pressure response to amlodipine among African-American men and women with early hypertensive renal disease
- PMID: 19907160
- PMCID: PMC2853591
- DOI: 10.1159/000258688
CYP3A4 and CYP3A5 polymorphisms and blood pressure response to amlodipine among African-American men and women with early hypertensive renal disease
Abstract
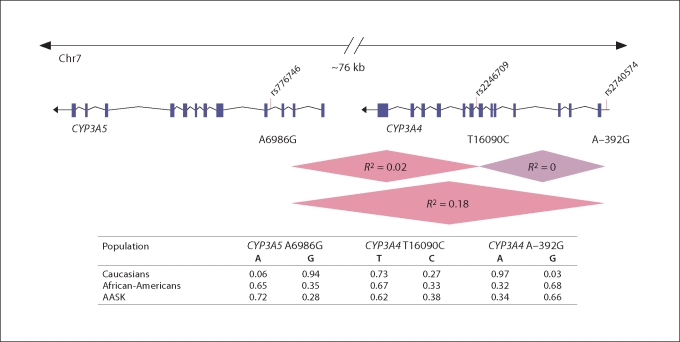
Purpose: To explore the association between CYP3A4 and CYP3A5 gene polymorphisms and blood pressure response to amlodipine among participants from the African-American Study of Kidney Disease and Hypertension Trial randomized to amlodipine (n = 164).
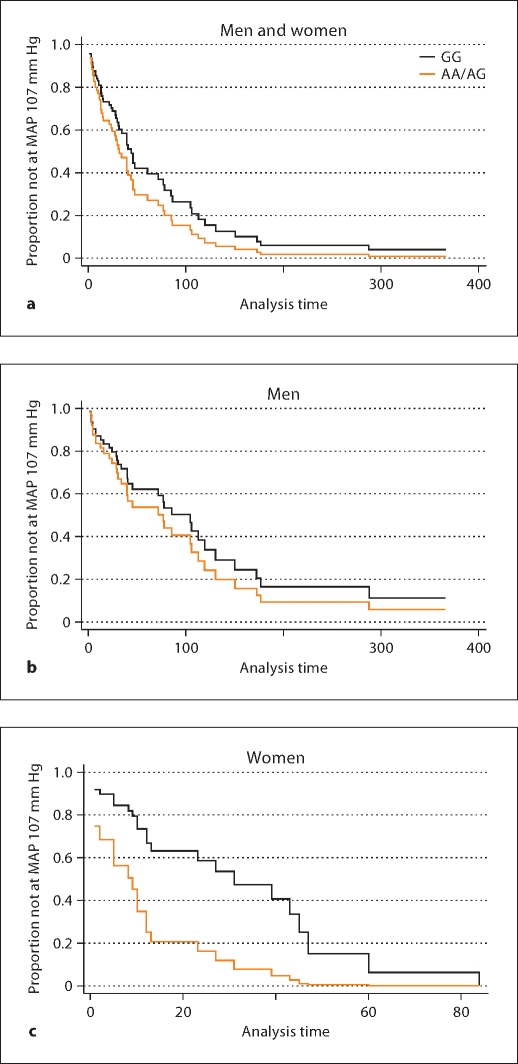
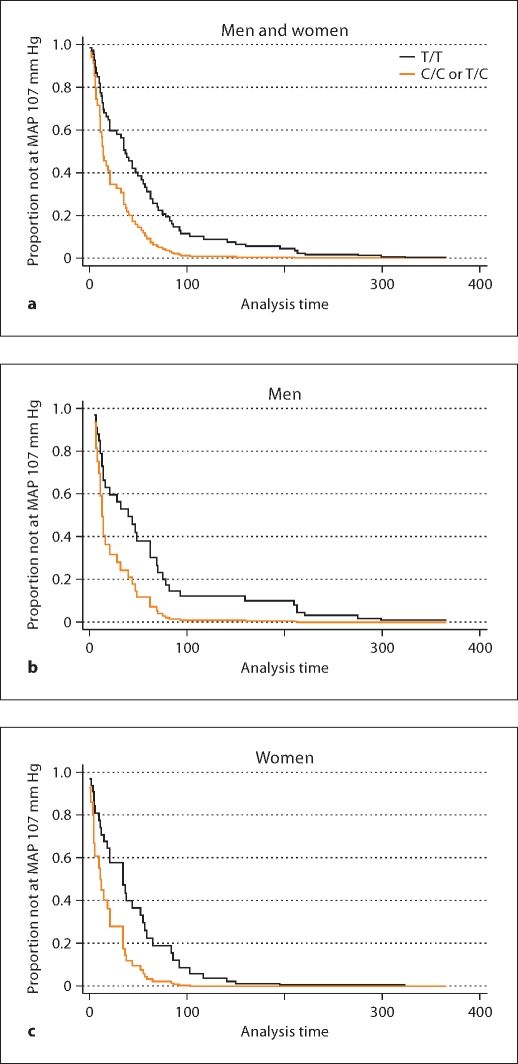
Methods: Cox proportional hazards models were used to determine the risk of reaching a target mean arterial pressure (MAP) of < or =107 mm Hg by CYP3A4 (A-392G and T16090C) and CYP3A5 (A6986G) gene polymorphisms, stratified by MAP randomization group (low or usual) and controlling for other predictors for blood pressure response.
Results: Women randomized to a usual MAP goal with an A allele at CYP3A4 A-392G were more likely to reach a target MAP of 107 mm Hg. The adjusted hazard ratio (AA/AG compared to GG) with 95% confidence interval was 3.41 (1.20-9.64; p = 0.020). Among participants randomized to a lower MAP goal, those with the C allele at CYP3A4 T16090C were more likely to reach target MAP: The adjusted hazard ratio was 2.04 (1.17-3.56; p = 0.010). After adjustment for multiple testing using a threshold significance level of p = 0.016, only the CYP3A4 T16090C SNP remained significant. CYP3A5 A6986G was not associated with blood pressure response.
Conclusions: Our findings suggest that blood pressure response to amlodipine among high-risk African-Americans appears to be determined by CYP3A4 genotypes, and sex specificity may be an important consideration. Clinical applications of CYP3A4 genotype testing for individualized treatment regimens warrant further study.
Copyright (c) 2009 S. Karger AG, Basel.
Figures
Similar articles
-
CYP3A4*1G and CYP3A5*3 genetic polymorphisms alter the antihypertensive efficacy of amlodipine in patients with hypertension following renal transplantation .Int J Clin Pharmacol Ther. 2017 Feb;55(2):109-118. doi: 10.5414/CP202559. Int J Clin Pharmacol Ther. 2017. PMID: 27841150
-
Association of the ADRB2 (rs2053044) polymorphism and angiotensin-converting enzyme-inhibitor blood pressure response in the African American Study of Kidney Disease and Hypertension.Pharmacogenet Genomics. 2015 Sep;25(9):444-9. doi: 10.1097/FPC.0000000000000154. Pharmacogenet Genomics. 2015. PMID: 26111150 Clinical Trial.
-
CYP3A5 polymorphism, amlodipine and hypertension.J Hum Hypertens. 2014 Mar;28(3):145-9. doi: 10.1038/jhh.2013.67. Epub 2013 Jul 18. J Hum Hypertens. 2014. PMID: 23863802 Review.
-
Successful blood pressure control in the African American Study of Kidney Disease and Hypertension.Arch Intern Med. 2002 Jul 22;162(14):1636-43. doi: 10.1001/archinte.162.14.1636. Arch Intern Med. 2002. PMID: 12123409 Clinical Trial.
-
Effect of CYP3A and ABCB1 single nucleotide polymorphisms on the pharmacokinetics and pharmacodynamics of calcineurin inhibitors: Part I.Clin Pharmacokinet. 2010 Mar;49(3):141-75. doi: 10.2165/11317350-000000000-00000. Clin Pharmacokinet. 2010. PMID: 20170205 Review.
Cited by
-
Identification of potential candidate genes for hypertensive nephropathy based on gene expression profile.BMC Nephrol. 2016 Oct 18;17(1):149. doi: 10.1186/s12882-016-0366-8. BMC Nephrol. 2016. PMID: 27756246 Free PMC article.
-
Effects of genetic factors on the pharmacokinetics and pharmacodynamics of amlodipine in primary hypertensive patients.Biomed Rep. 2015 Mar;3(2):195-200. doi: 10.3892/br.2014.395. Epub 2014 Dec 2. Biomed Rep. 2015. PMID: 26075072 Free PMC article.
-
A review of clinical pharmacogenetics Studies in African populations.Per Med. 2020 Mar;17(2):155-170. doi: 10.2217/pme-2019-0110. Epub 2020 Mar 3. Per Med. 2020. PMID: 32125935 Free PMC article. Review.
-
The influence of comedication on tacrolimus blood concentration in patients subjected to kidney transplantation: a retrospective study.Eur J Drug Metab Pharmacokinet. 2014 Dec;39(4):243-53. doi: 10.1007/s13318-013-0168-3. Epub 2013 Dec 20. Eur J Drug Metab Pharmacokinet. 2014. PMID: 24356808
-
Association of CYP3A5 Gene Polymorphisms and Amlodipine-Induced Peripheral Edema in Chinese Han Patients with Essential Hypertension.Pharmgenomics Pers Med. 2021 Feb 2;14:189-197. doi: 10.2147/PGPM.S291277. eCollection 2021. Pharmgenomics Pers Med. 2021. PMID: 33564260 Free PMC article.
References
-
- Rizzo JA, Simons WR. Variations in compliance among hypertensive patients by drug class: implications for health care costs. Clin Ther. 1997;19:1446–1457. - PubMed
-
- Appel LJ, et al. The rationale and design of the AASK cohort study. J Am Soc Nephrol. 2003;14(suppl 2):S166–S172. - PubMed
-
- Chobanian AV, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 Report. JAMA. 2003;289:2560–2572. - PubMed
-
- McClellan W, Tuttle E, Issa A. Racial differences in the incidence of hypertensive end-stage renal disease are not entirely explained by differences in the prevalence of hypertension. Am J Kidney Dis. 1988;12:285–290. - PubMed
-
- Safford MM, et al. Understanding racial disparities in hypertension control: intensity of hypertension medication treatment in the REGARDS study. Ethn Dis. 2007;17:421–426. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- RR11145/RR/NCRR NIH HHS/United States
- K23 RR020822/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- R01 DK060702/DK/NIDDK NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- DK60702/DK/NIDDK NIH HHS/United States
- U01 DK048689/DK/NIDDK NIH HHS/United States
- DK057867/DK/NIDDK NIH HHS/United States
- P60 MD000220/MD/NIMHD NIH HHS/United States
- P20 RR011145/RR/NCRR NIH HHS/United States
- RR00827/RR/NCRR NIH HHS/United States
- R01 DK057867/DK/NIDDK NIH HHS/United States
- K23 RR020822-01A1/RR/NCRR NIH HHS/United States
- RR000071/RR/NCRR NIH HHS/United States
- DK048689/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
