

Severe sepsis in two Ugandan hospitals: a prospective observational study of management and outcomes in a predominantly HIV-1 infected population
- PMID: 19907656
- PMCID: PMC2771355
- DOI: 10.1371/journal.pone.0007782
Severe sepsis in two Ugandan hospitals: a prospective observational study of management and outcomes in a predominantly HIV-1 infected population
Abstract
Background: Sepsis likely contributes to the high burden of infectious disease morbidity and mortality in low income countries. Data regarding sepsis management in sub-Saharan Africa are limited. We conducted a prospective observational study reporting the management and outcomes of severely septic patients in two Ugandan hospitals. We describe their epidemiology, management, and clinical correlates for mortality.
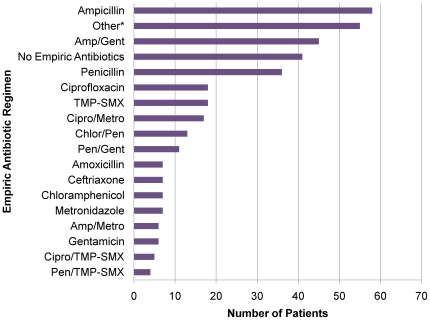
Methodology/results: Three-hundred eighty-two patients fulfilled enrollment criteria for a severe sepsis syndrome. Vital signs, management and laboratory results were recorded. Outcomes measured included in-hospital and post-discharge mortality. Most patients were HIV-infected (320/377, 84.9%) with a median CD4+ T cell (CD4) count of 52 cells/mm(3) (IQR, 16-131 cells/mm(3)). Overall mortality was 43.0%, with 23.7% in-hospital mortality (90/380) and 22.3% post-discharge mortality (55/247). Significant predictors of in-hospital mortality included admission Glasgow Coma Scale and Karnofsky Performance Scale (KPS), tachypnea, leukocytosis and thrombocytopenia. Discharge KPS and early fluid resuscitation were significant predictors of post-discharge mortality. Among HIV-infected patients, CD4 count was a significant predictor of post-discharge mortality. Median volume of fluid resuscitation within the first 6 hours of presentation was 500 mLs (IQR 250-1000 mls). Fifty-two different empiric antibacterial regimens were used during the study. Bacteremic patients were more likely to die in hospital than non-bacteremic patients (OR 1.83, 95% CI = 1.01-3.33). Patients with Mycobacterium tuberculosis (MTB) bacteremia (25/249) had higher in-hospital mortality (OR 1.97, 95% CI = 1.19-327) and lower median CD4 counts (p = 0.001) than patients without MTB bacteremia.
Conclusion: Patients presenting with sepsis syndromes to two Ugandan hospitals had late stage HIV infection and high mortality. Bacteremia, especially from MTB, was associated with increased in-hospital mortality. Most clinical predictors of in-hospital mortality were easily measurable and can be used for triaging patients in resource-constrained settings. Procurement of low cost and high impact treatments like intravenous fluids and empiric antibiotics may help decrease sepsis-associated mortality in resource-constrained settings.
Conflict of interest statement
Figures


References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med. 2003;348:138–150. - PubMed
-
- Archibald LK, den Dulk MO, Pallangyo KJ, Reller LB. Fatal Mycobacterium tuberculosis bloodstream infections in febrile hospitalized adults in Dar es Salaam, Tanzania. Clin Infect Dis. 1998;26:290–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
