

Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients
- PMID: 19908092
- PMCID: PMC2841280
- DOI: 10.1007/s00270-009-9727-z
Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients
Abstract
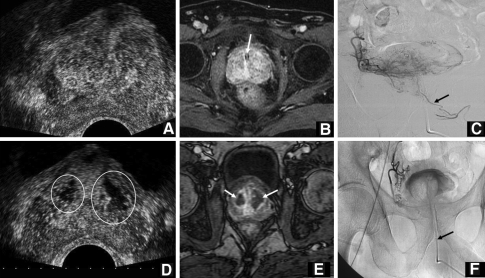
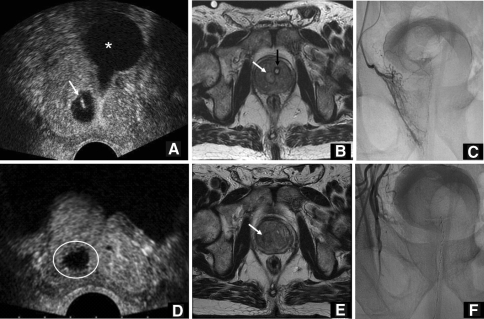
Symptomatic benign prostatic hyperplasia (BPH) typically occurs in the sixth and seventh decades, and the most frequent obstructive urinary symptoms are hesitancy, decreased urinary stream, sensation of incomplete emptying, nocturia, frequency, and urgency. Various medications, specifically 5-alpha-reductase inhibitors and selective alpha-blockers, can decrease the severity of the symptoms secondary to BPH, but prostatectomy is still considered to be the traditional method of management. We report the preliminary results for two patients with acute urinary retention due to BPH, successfully treated by prostate artery embolization (PAE). The patients were investigated using the International Prostate Symptom Score, by digital rectal examination, urodynamic testing, prostate biopsy, transrectal ultrasound (US), and magnetic resonance imaging (MRI). Uroflowmetry and postvoid residual urine volume complemented the investigation at 30, 90, and 180 days after PAE. The procedure was performed under local anesthesia; embolization of the prostate arteries was performed with a microcatheter and 300- to 500-microm microspheres using complete stasis as the end point. One patient was subjected to bilateral PAE and the other to unilateral PAE; they urinated spontaneously after removal of the urethral catheter, 15 and 10 days after the procedure, respectively. At 6-month follow-up, US and MRI revealed a prostate reduction of 39.7% and 47.8%, respectively, for the bilateral PAE and 25.5 and 27.8%, respectively, for the patient submitted to unilateral PAE. The early results, at 6-month follow-up, for the two patients with BPH show a promising potential alternative for treatment with PAE.
Figures
References
-
- AUA Practice Guidelines Committee AUA guideline on management of benign prostatic hyperplasia. I. Diagnosis and treatment recommendations. J Urol. 2003;170(2; pt 1):530–547. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
