

Relapse in resected lung cancer revisited: does intensified follow up really matter? A prospective study
- PMID: 19909550
- PMCID: PMC2784765
- DOI: 10.1186/1477-7819-7-87
Relapse in resected lung cancer revisited: does intensified follow up really matter? A prospective study
Abstract
Background: beside the well known predominance of distant vs. loco-regional relapse, several aspects of the relapse pattern still have not been fully elucidated.
Methods: prospective, controlled study on 88 patients operated for non-small cell lung cancer (NSCLC) in a 15 months period. Stage IIIA existed in 35(39.8%) patients, whilst stages IB, IIA and IIB existed in 10.2%, 4.5% and 45.5% patients respectively.
Inclusion criteria: stage I-IIIA, complete resection, systematic lymphadenectomy with at least 6 lymph node groups examined, no neoadjuvant therapy, exact data of all aspects of relapse, exact data about the outcome of the treatment.
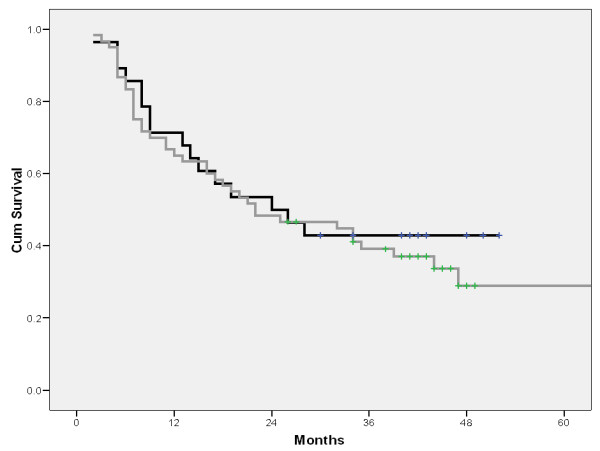
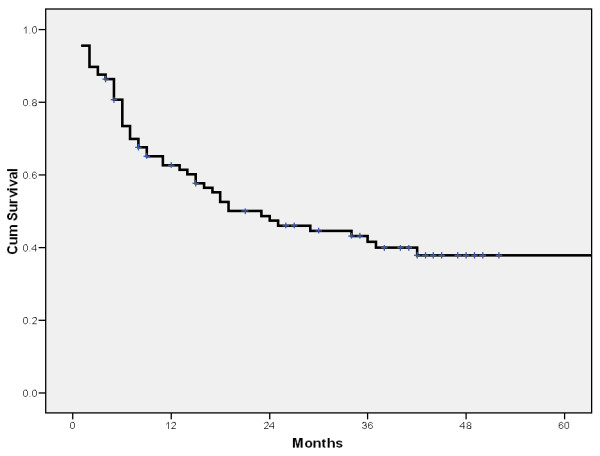
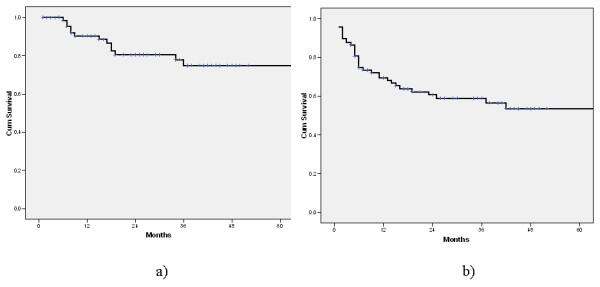
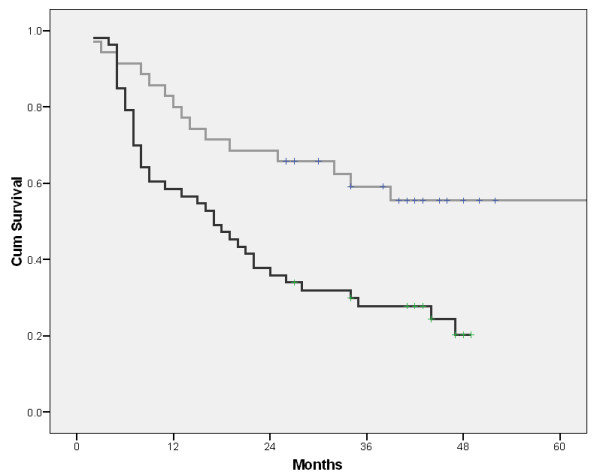
Results: postoperative lung cancer relapse occurred in 50(56.8%) patients. Locoregional, distant and both types of relapse occurred in 26%, 70% and 4% patients respectively. Postoperative cancer relapse occurred in 27/35(77.1%) pts. in the stage IIIA and in 21/40(52.55) pts in the stage IIB. In none of four pts. in the stage IIA cancer relapse occurred, unlike 22.22% pts. with relapse in the stage IB. The mean disease free interval in the analysed group was 34.38 +/- 3.26 months.The mean local relapse free and distant relapse free intervals were 55 +/- 3.32 and 41.62 +/- 3.47 months respectively Among 30 pts. with the relapse onset inside the first 12 month after the lung resection, in 20(66.6%) pts. either T3 tumours or N2 lesions existed. In patients with N0, N1 and N2 lesions, cancer relapse occurred in 30%, 55.6% and 70.8% patients respectively. Radiographic aspect T stage, N stage and extent of resection were found as significant in terms of survival. Related to the relapse occurrence, although radiographic aspect and extent of resection followed the same trend as in the survival analysis, only T stage and N stage were found as significant in the same sense as for survival. On multivariate, only T and N stage were found as significant in terms of survival.Specific oncological treatment of relapse was possible in 27/50(54%) patients.
Conclusion: the intensified follow up did not increase either the proportion of patients detected with asymptomatic relapse or the number of patients with specific oncological treatment of relapse.
Figures
References
-
- Martini N, Burt ME, Bains MS, McCormack PM, Rusch VW, Ginsberg RJ. Survival after resection of stage II non-small cell lung cancer. Ann Thorac Surg. 1992;54:460–6. - PubMed
-
- Yano T, Yokoyama H, Inoue T, Asoh H, Tayama K, Ichinose Y. Surgical results and prognostic factors of pathologic N1 disease in non-small cell carcinoma of the lung. Significance of N1 level: lobar or hilar nodes. J Thorac Cardiovasc Surg. 1994;107:1398–1402. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
