

Brain immaturity is associated with brain injury before and after neonatal cardiac surgery with high-flow bypass and cerebral oxygenation monitoring
- PMID: 19909994
- PMCID: PMC2827639
- DOI: 10.1016/j.jtcvs.2009.08.022
Brain immaturity is associated with brain injury before and after neonatal cardiac surgery with high-flow bypass and cerebral oxygenation monitoring
Abstract
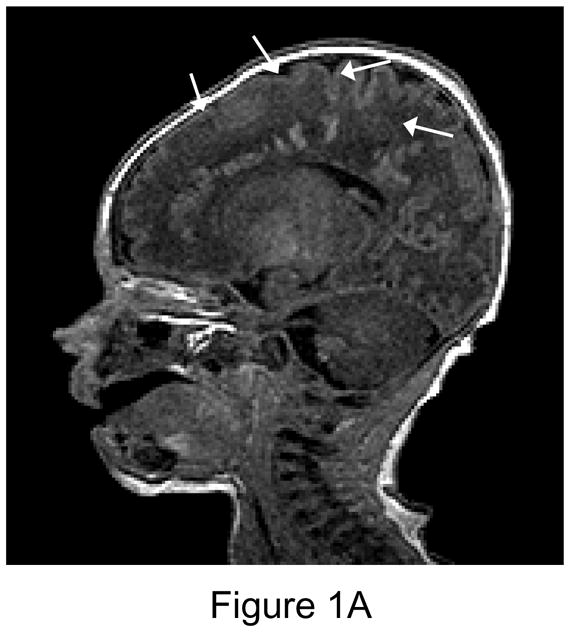
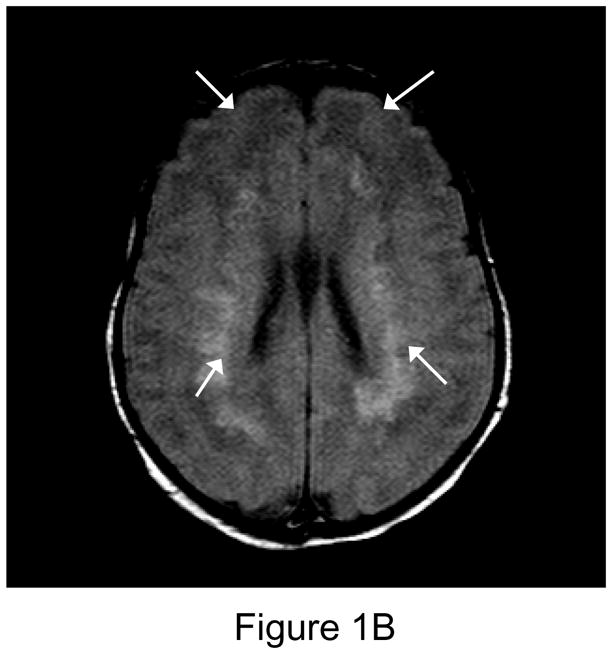
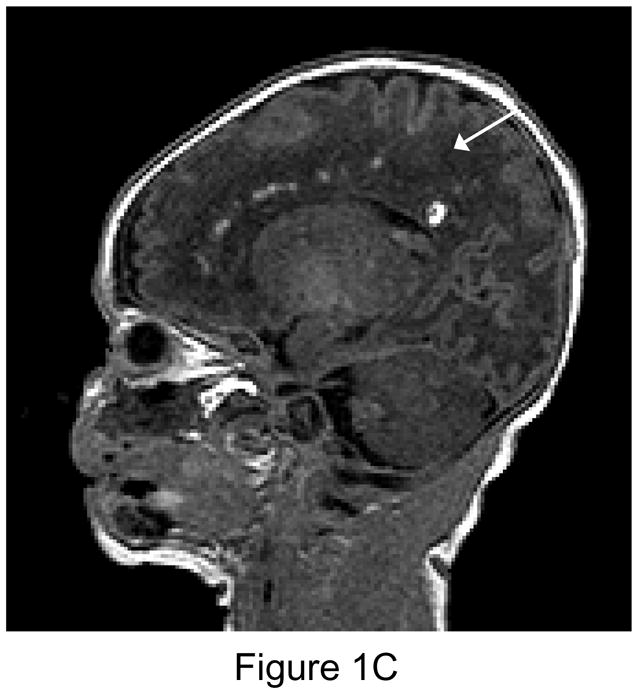
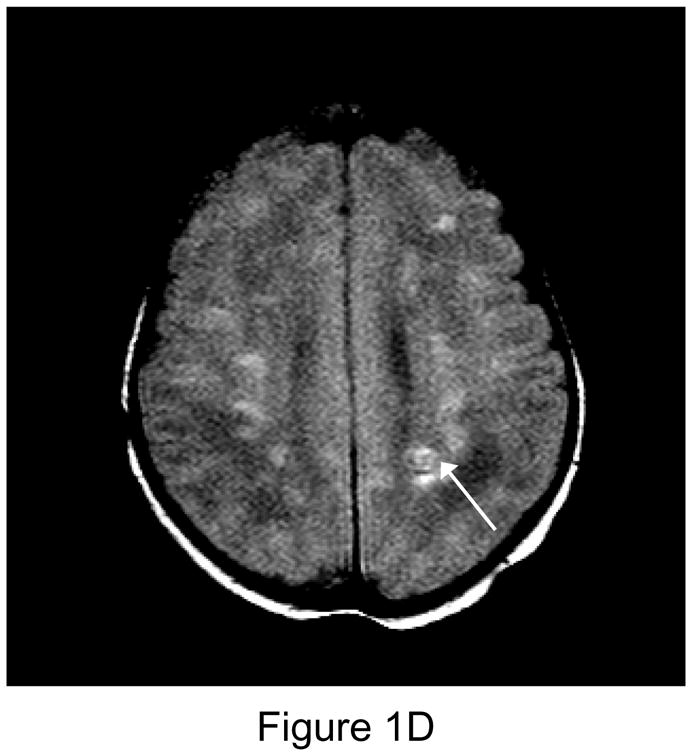
Background: New intraparenchymal brain injury on magnetic resonance imaging is observed in 36% to 73% of neonates after cardiac surgery with cardiopulmonary bypass. Brain immaturity in this population is common. We performed brain magnetic resonance imaging before and after neonatal cardiac surgery, using a high-flow cardiopulmonary bypass protocol, hypothesizing that brain injury on magnetic resonance imaging would be associated with brain immaturity.
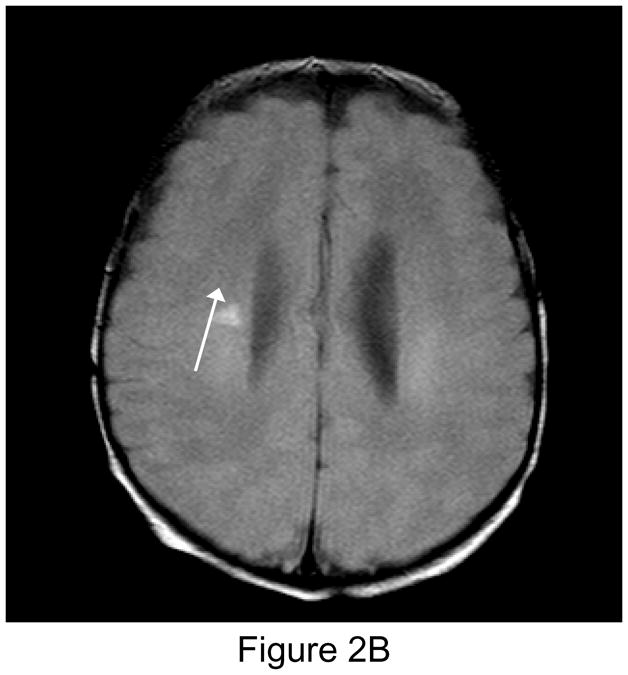
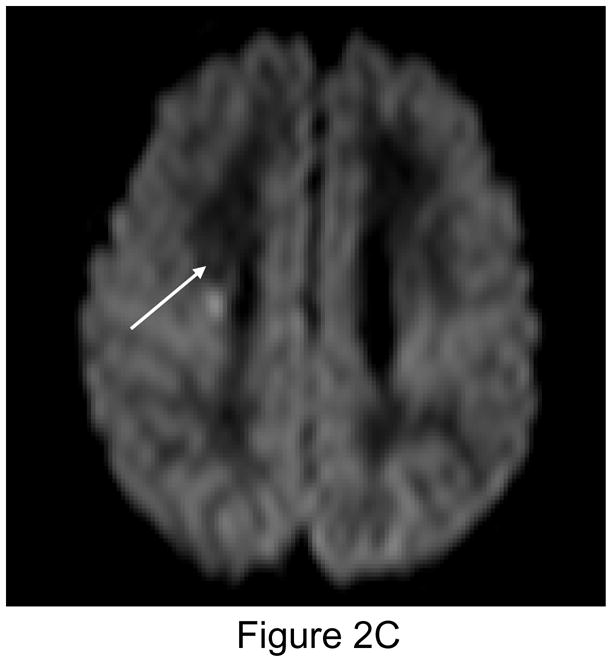
Methods: Cardiopulmonary bypass protocol included 150 mL . kg(-1) . min(-1) flows, pH stat management, hematocrit > 30%, and high-flow antegrade cerebral perfusion. Regional brain oxygen saturation was monitored, with a treatment protocol for regional brain oxygen saturation < 50%. Brain magnetic resonance imaging, consisting of T1-, T2-, and diffusion-weighted imaging, and magnetic resonance spectroscopy were performed preoperatively, 7 days postoperatively, and at age 3 to 6 months.
Results: Twenty-four of 67 patients (36%) had new postoperative white matter injury, infarction, or hemorrhage, and 16% had new white matter injury. Associations with preoperative brain injury included low brain maturity score (P = .002). Postoperative white matter injury was associated with single-ventricle diagnosis (P = .02), preoperative white matter injury (P < .001), and low brain maturity score (P = .05). Low brain maturity score was also associated with more severe postoperative brain injury (P = .01). Forty-five patients had a third scan, with a 27% incidence of new minor lesions, but 58% of previous lesions had partially or completely resolved.
Conclusions: We observed a significant incidence of both pre- and postoperative magnetic resonance imaging abnormality and an association with brain immaturity. Many lesions resolved in the first 6 months after surgery. Timing of delivery and surgery with bypass could affect the risk of brain injury.
Copyright 2010 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Welke KF, Shen I, Ungerleider RM. Current assessment of mortality rates in congenital cardiac surgery. Ann Thorac Surg. 2006;82:164–71. - PubMed
-
- Wernovsky G, Shillingford AJ, Gaynor JW. Central nervous system outcomes in children with complex congenital heart disease. Curr Opin Cardiol. 2005;20:94–99. - PubMed
-
- Creighton DE, Robertson CM, Sauve RS, Moddemann DM, Alton GY, Nettel-Aguirre A, et al. Neurocognitive, functional, and health outcomes at 5 years of age for children after complex cardiac surgery at 6 weeks of age or younger. Pediatrics. 2007;120:e478–86. - PubMed
-
- Majnemer A, Limperopoulos C, Shevell M, Rosenblatt B, Rohlicek C, Tchervenkov C. Long-term neuromotor outcome at school entry of infants with congenital heart defects requiring open-heart surgery. J Pediatr. 2006;148:72–7. - PubMed
-
- Dent CL, Spaeth JP, Jones BV, Schwartz SM, Glauser TA, Hallinan B, et al. Brain magnetic resonance imaging abnormalities after the Norwood procedure using regional cerebral perfusion. J Thorac Cardiovasc Surg. 2006;131:190–97. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
