

Murine model of surgically induced acute aortic dissection type A
- PMID: 19910001
- PMCID: PMC3454491
- DOI: 10.1016/j.jtcvs.2009.08.039
Murine model of surgically induced acute aortic dissection type A
Abstract
Objectives: This study aimed at developing a murine model of surgically induced acute aortic dissection type A for investigation of the formation and progression of acute aortic dissection and to test whether this system could be used for biomarker discovery.
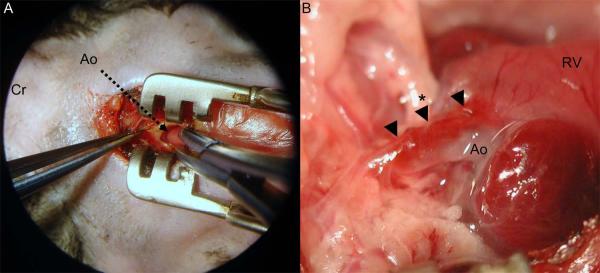
Methods: Adult fibrillin-1 deficient, Fbn1(C1039G/+) mice and wild-type mice were anesthetized, ventilated, and the ascending aorta exposed via hemisternotomy. We hypothesized that acute aortic dissection could be induced either by injecting autologous blood into the aortic wall or by injury to the wall with aortic clamping. Echocardiography was done preoperatively, and serum samples were collected before and 30 minutes after the operation and analyzed by enzyme-linked immunosorbent assay.
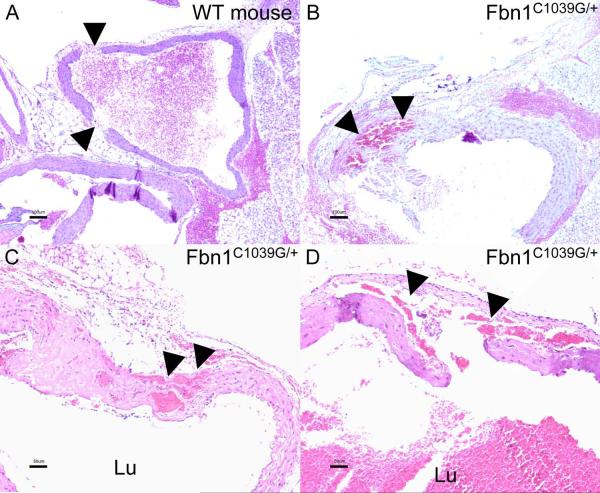
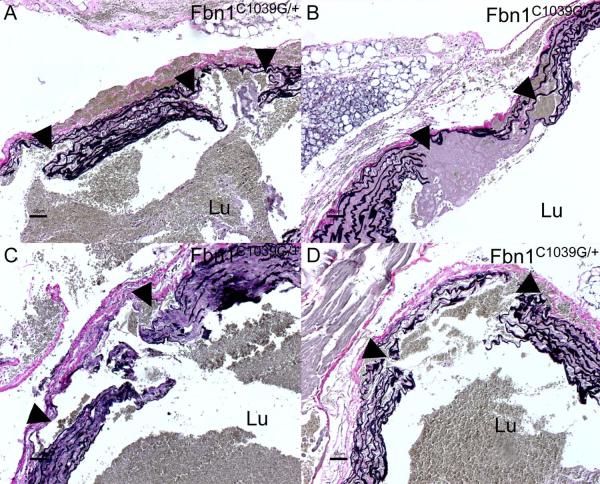
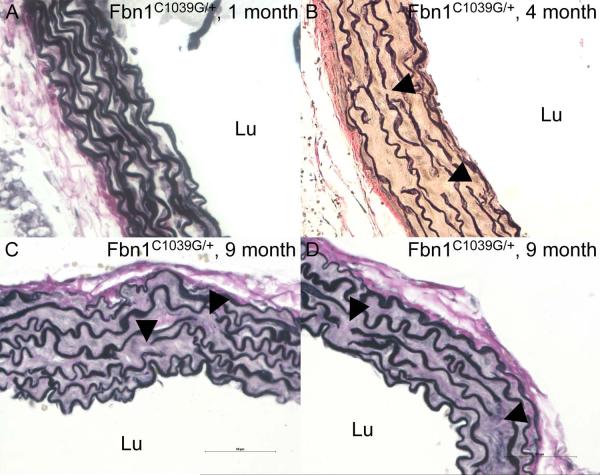
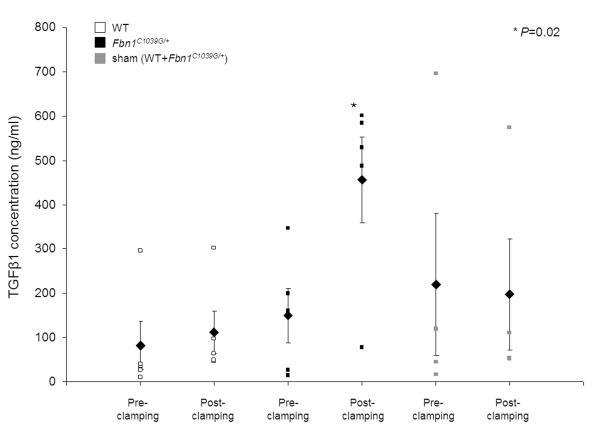
Results: Echocardiography revealed larger aortic root diameters in Fbn1(C1039G/+) compared with wild-type mice (P = .001). Histologic examination showed that aortic clamp injury but not injection of blood leads to large intimal tears, disruption of aortic wall structures, and localized dissection of the aortic media in Fbn1(C1039G/+) mice. Acute aortic dissection developed in 4 of 5 Fbn1(C1039G/+) mice versus 0 of 5 wild-type mice after aortic clamping (P < .01). Elastin staining showed higher elastic fiber fragmentation and disarray in Fbn1(C1039G/+) compared with wild-type mice. Enzyme-linked immunosorbent assay analysis revealed elevated circulating transforming growth factor beta1 concentrations after induction of acute aortic dissection in Fbn1(C1039G/+) mice (P = .02, 150 +/- 61 ng/mL vs 456 +/- 97 ng/mL), but not in wild-type or sham-operated mice.
Conclusions: Aortic clamp injury can induce AAD in Fbn1(C1039G/+), but not in wild-type mice. This murine model of surgically induced acute aortic dissection is highly reproducible and nonlethal in the short term. Using this system, we revealed that circulating transforming growth factor beta1 is a promising biomarker for acute aortic dissection.
Copyright 2010 The American Association for Thoracic Surgery. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Hagan PG, Nienaber CA, Isselbacher EM, Bruckman D, Karavite DJ, Russman PL, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. Jama. 2000;283:897–903. - PubMed
-
- Masuda Y, Yamada Z, Morooka N, Watanabe S, Inagaki Y. Prognosis of patients with medically treated aortic dissections. Circulation. 1991;84:III7–13. - PubMed
-
- Marsalese DL, Moodie DS, Lytle BW, Cosgrove DM, Ratliff NB, Goormastic M, et al. Cystic medial necrosis of the aorta in patients without Marfan’s syndrome: surgical outcome and long-term follow-up. J Am Coll Cardiol. 1990;16:68–73. - PubMed
-
- Svensson LG, Crawford ES. Aortic dissection and aortic aneurysm surgery: clinical observations, experimental investigations, and statistical analyses. Part II. Curr Probl Surg. 1992;29:913–1057. - PubMed
-
- Matt P, Habashi J, Carrel T, Cameron DE, Van Eyk JE, Dietz HC. Recent advances in understanding Marfan syndrome: should we now treat surgical patients with losartan? J Thorac Cardiovasc Surg. 2008;135:389–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
