

Fluorodeoxyglucose-positron-emission tomography imaging of head and neck squamous cell cancer
- PMID: 19910448
- PMCID: PMC7964245
- DOI: 10.3174/ajnr.A1760
Fluorodeoxyglucose-positron-emission tomography imaging of head and neck squamous cell cancer
Abstract
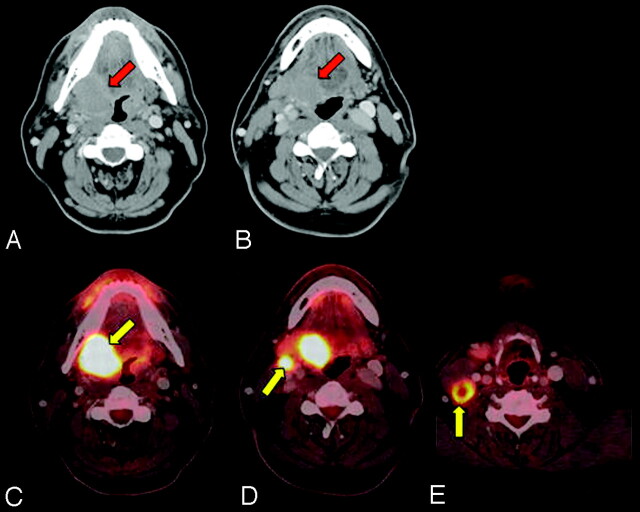
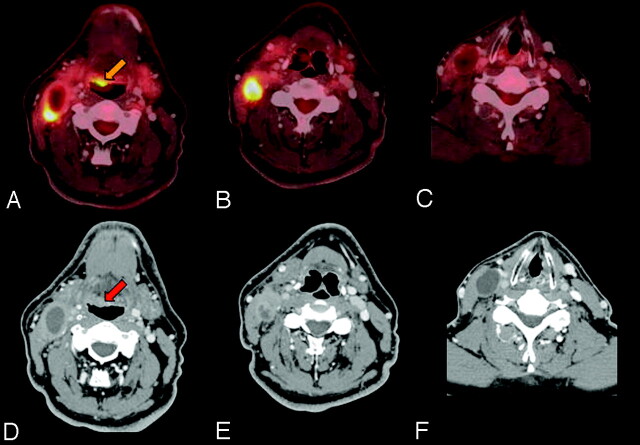
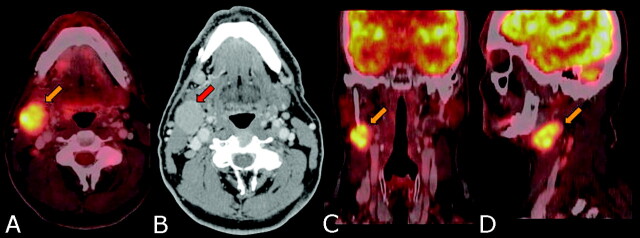
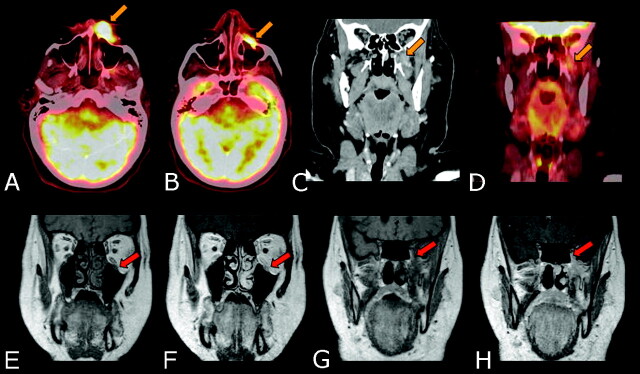
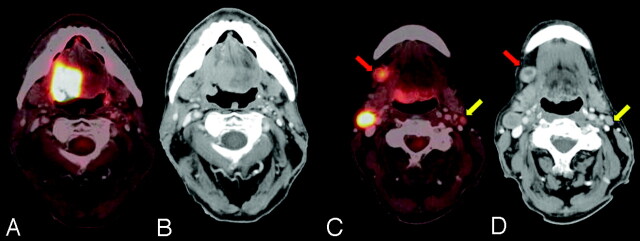
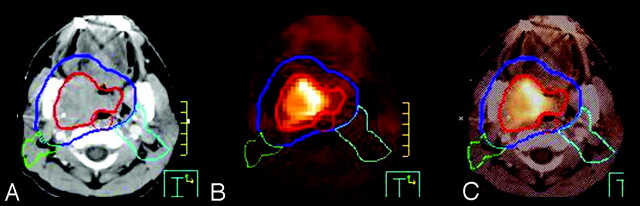
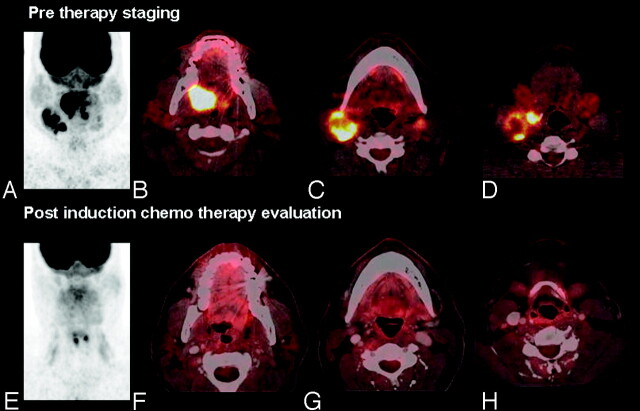
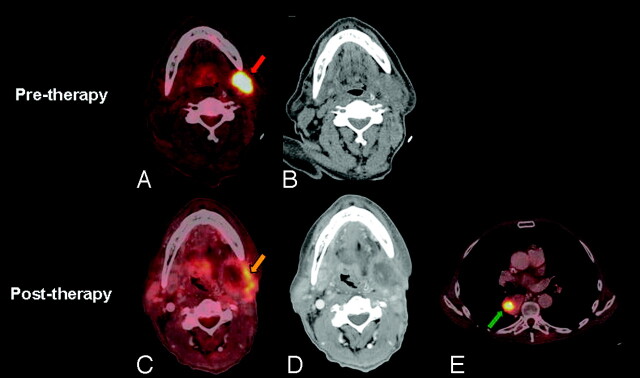
The hybrid technique of PET/CT has significantly impacted the imaging and management of HNSCC since its introduction in 2001 and has become the technique of choice for imaging of this cancer. Diagnostic FDG-PET/CT is useful for identification of an unknown primary tumor, delineation of extent of primary tumor, detection of regional lymph node involvement even in a normal-sized node, detection of distant metastases and occasional synchronous primary tumor, assessment of therapy response, and long-term surveillance for recurrence and metastases. The role of PET/CT is evolving in radiation therapy planning. Combined diagnostic PET/CT provides the best anatomic and metabolic in vivo information for the comprehensive management of HNSCC.
Figures
Similar articles
-
Positron emission tomography-computed tomography surveillance for the node-positive neck after chemoradiotherapy.Laryngoscope. 2009 Jun;119(6):1120-4. doi: 10.1002/lary.20201. Laryngoscope. 2009. PMID: 19358193
-
Evaluation of the therapeutic effects and recurrence for head and neck cancer after chemoradiotherapy by FDG-PET.Auris Nasus Larynx. 2009 Apr;36(2):192-8. doi: 10.1016/j.anl.2008.05.009. Epub 2008 Jul 7. Auris Nasus Larynx. 2009. PMID: 18606510
-
[Correlation of FDG-PET and MRI/CT with histopathology in primary diagnosis, lymph node staging and diagnosis of recurrency of head and neck cancer].Rofo. 2002 Jun;174(6):714-20. doi: 10.1055/s-2002-32215. Rofo. 2002. PMID: 12063600 German.
-
[Post-therapeutic imaging strategies and follow-up in head and neck malignant tumours].HNO. 2010 Aug;58(8):749-55. doi: 10.1007/s00106-010-2143-5. HNO. 2010. PMID: 20640391 Review. German.
-
Role of PET FDG in the management of head and neck squamous cell cancer.Clin Oncol (R Coll Radiol). 1998;10(6):361-6. doi: 10.1016/s0936-6555(98)80030-7. Clin Oncol (R Coll Radiol). 1998. PMID: 9890536 Review. No abstract available.
Cited by
-
No benefit for regional control and survival by planned neck dissection in primary irradiated oropharyngeal cancer irrespective of p16 expression.Eur Arch Otorhinolaryngol. 2016 Jul;273(7):1841-8. doi: 10.1007/s00405-015-3675-9. Epub 2015 Jun 10. Eur Arch Otorhinolaryngol. 2016. PMID: 26059208
-
The role of FDG PET-CT in the therapeutic evaluation for HNSCC patients.Jpn J Radiol. 2012 Jul;30(6):463-70. doi: 10.1007/s11604-012-0076-5. Epub 2012 Apr 5. Jpn J Radiol. 2012. PMID: 22476892 Review.
-
Current oncologic concepts and emerging techniques for imaging of head and neck squamous cell cancer.GMS Curr Top Otorhinolaryngol Head Neck Surg. 2012;11:Doc08. doi: 10.3205/cto000090. Epub 2012 Dec 20. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2012. PMID: 23320060 Free PMC article.
-
Changes in Apparent Diffusion Coefficient (ADC) in Serial Weekly MRI during Radiotherapy in Patients with Head and Neck Cancer: Results from the PREDICT-HN Study.Curr Oncol. 2022 Aug 31;29(9):6303-6313. doi: 10.3390/curroncol29090495. Curr Oncol. 2022. PMID: 36135064 Free PMC article.
-
PKM2 Modulation in Head and Neck Squamous Cell Carcinoma.Int J Mol Sci. 2022 Jan 11;23(2):775. doi: 10.3390/ijms23020775. Int J Mol Sci. 2022. PMID: 35054968 Free PMC article.
References
-
- Carvalho A, Nishimoto I, Califano J, et al. . Trends in incidence and prognosis for head and neck cancer in the United States: a site-specific analysis of the SEER database. Int J Cancer 2005; 114: 806–16 - PubMed
-
- Canto MT, Devesa SS. Oral cavity and pharynx cancer incidence rates in the United States, 1975–1998. Oral Oncol 2002; 38: 610–17 - PubMed
-
- Forastiere A, Koch W, Trotti A, et al. . Head and neck cancer. N Engl J Med 2001; 345: 1890–900 - PubMed
-
- Cooper JS, Pajak TF, Forastiere AA, et al. . Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med 2004; 350: 1937–44 - PubMed
-
- Bernier J, Domenge C, Ozsahin M, et al. . Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med 2004; 350: 1945–52 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical