

Reperfusion is a more accurate predictor of follow-up infarct volume than recanalization: a proof of concept using CT in acute ischemic stroke patients
- PMID: 19910542
- PMCID: PMC2909663
- DOI: 10.1161/STROKEAHA.109.568766
Reperfusion is a more accurate predictor of follow-up infarct volume than recanalization: a proof of concept using CT in acute ischemic stroke patients
Abstract
Background and purpose: The purpose of this study was to compare recanalization and reperfusion in terms of their predictive value for imaging outcomes (follow-up infarct volume, infarct growth, salvaged penumbra) and clinical outcome in acute ischemic stroke patients.
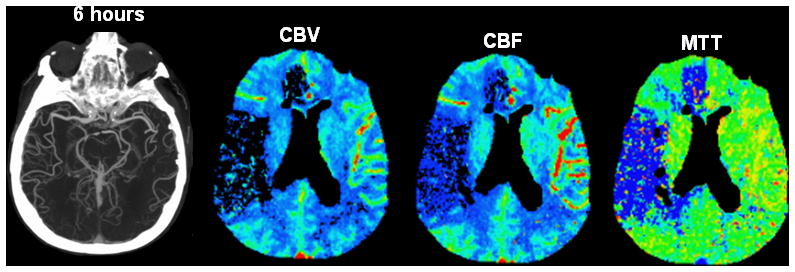
Material and methods: Twenty-two patients admitted within 6 hours of stroke onset were retrospectively included in this study. These patients underwent a first stroke CT protocol including CT-angiography (CTA) and perfusion-CT (PCT) on admission, and similar imaging after treatment, typically around 24 hours, to assess recanalization and reperfusion. Recanalization was assessed by comparing arterial patency on admission and posttreatment CTAs; reperfusion, by comparing the volumes of CBV, CBF, and MTT abnormality on admission and posttreatment PCTs. Collateral flow was graded on the admission CTA. Follow-up infarct volume was measured on the discharge noncontrast CT. The groups of patients with reperfusion, no reperfusion, recanalization, and no recanalization were compared in terms of imaging and clinical outcomes.
Results: Reperfusion (using an MTT reperfusion index >75%) was a more accurate predictor of follow-up infarct volume than recanalization. Collateral flow and recanalization were not accurate predictors of follow-up infarct volume. An interaction term was found between reperfusion and the volume of the admission penumbra >50 mL.
Conclusions: Our study provides evidence that reperfusion is a more accurate predictor of follow-up infarct volume in acute ischemic stroke patients than recanalization. We recommend an MTT reperfusion index >75% to assess therapy efficacy in future acute ischemic stroke trials that use perfusion-CT.
Figures








References
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- del Zoppo GJ, Koziol JA. Recanalization and stroke outcome. Circulation. 2007;115:2602–2605. - PubMed
-
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke. 2007;38:967–973. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
