

Effect of cardiopulmonary bypass on activated partial thromboplastin time waveform analysis, serum procalcitonin and C-reactive protein concentrations
- PMID: 19912638
- PMCID: PMC2811936
- DOI: 10.1186/cc8166
Effect of cardiopulmonary bypass on activated partial thromboplastin time waveform analysis, serum procalcitonin and C-reactive protein concentrations
Abstract
Introduction: Systemic inflammatory response syndrome (SIRS) is a frequent condition after cardiopulmonary bypass (CPB) and makes conventional biological tests fail to detect postoperative sepsis. Biphasic waveform (BPW) analysis is a new biological test derived from activated partial thromboplastin time that has recently been proposed for sepsis diagnosis. The aim of this study was to investigate the accuracy of BPW to detect sepsis after cardiac surgery under CPB.
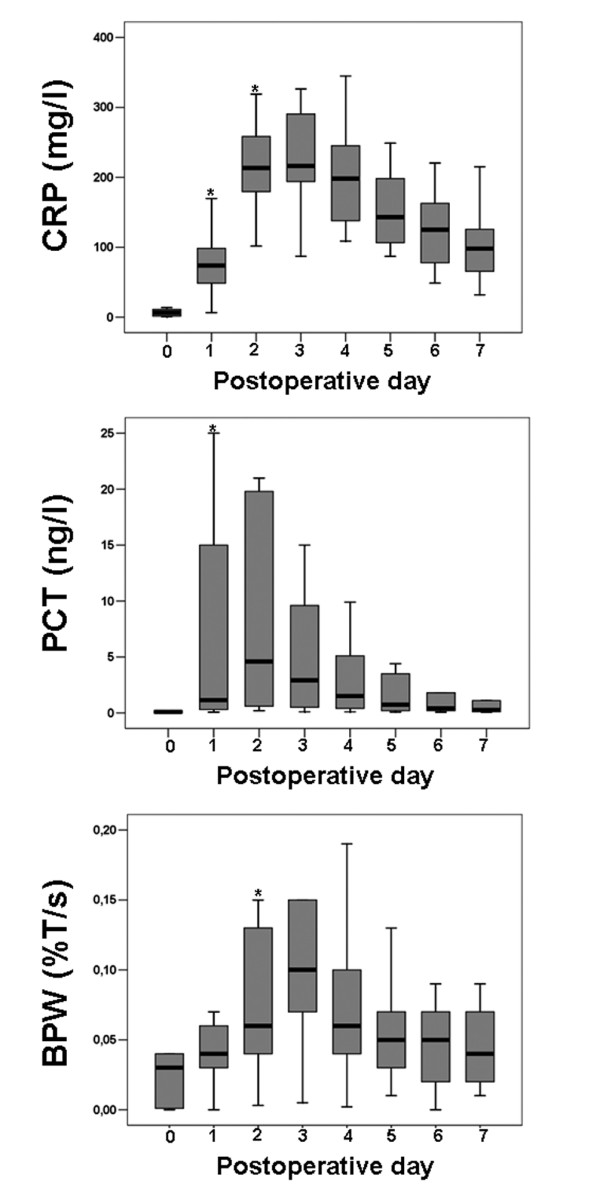
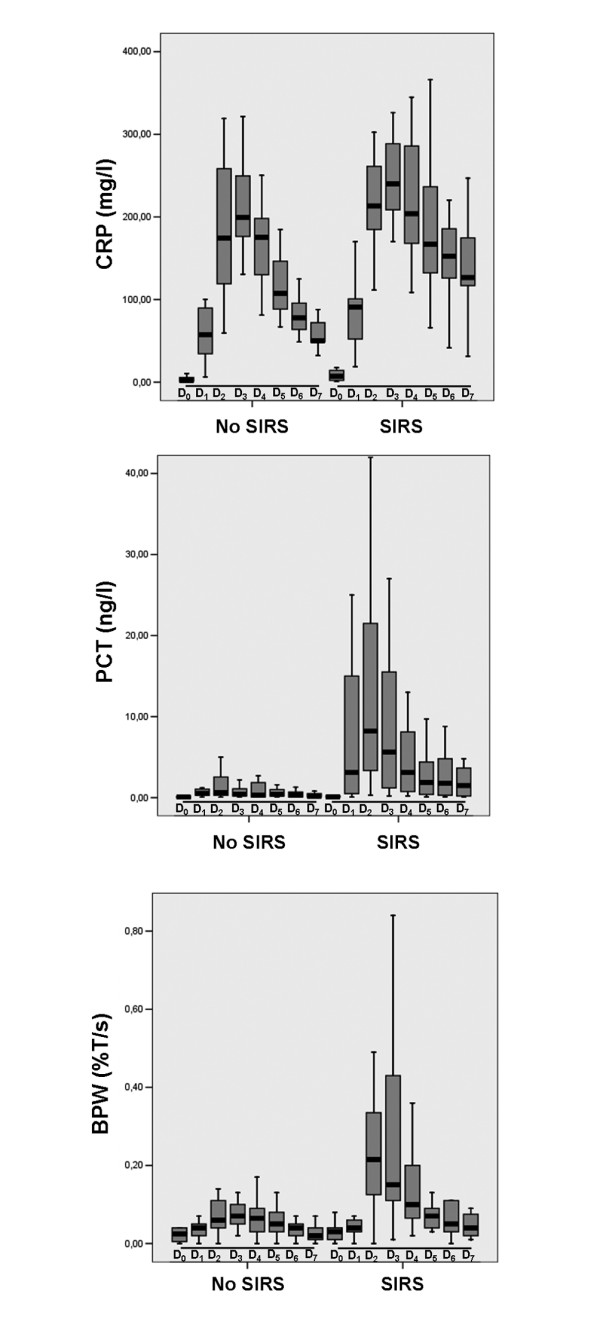
Methods: We conducted a prospective study in American Society of Anesthesiologists' (ASA) physical status III and IV patients referred for cardiac surgery under CPB. Procalcitonin (PCT) and BPW were recorded before surgery and every day during the first week following surgery. Patients were then divided into three groups: patients presenting no SIRS, patients presenting with non-septic SIRS and patients presenting with sepsis.
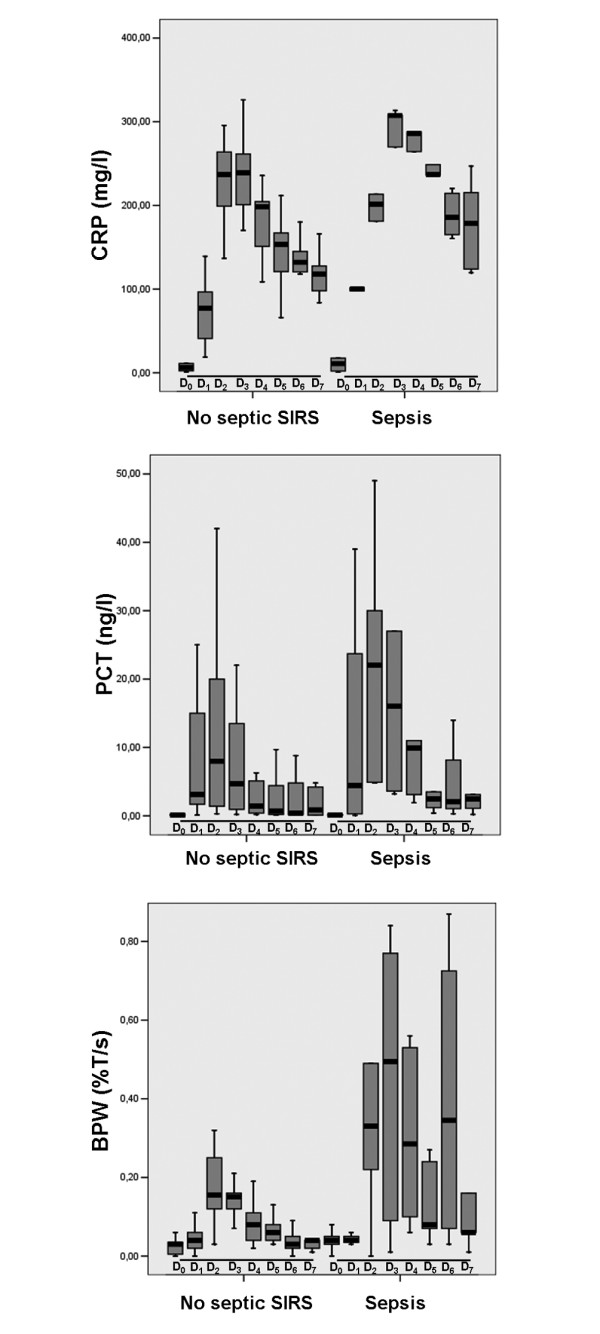
Results: Thirty two patients were included. SIRS occurred in 16 patients (50%) including 5 sepsis (16%) and 11 (34%) non-septic SIRS. PCT and BPW were significantly increased in SIRS patients compared to no SIRS patients (0.9 [0.5-2.2] vs. 8.1 [2.0-21.3] ng/l for PCT and 0.10 [0.09-0.14] vs. 0.29 [0.16-0.56] %T/s for BPW; P < 0.05 for both). We observed no difference in peak PCT value between the sepsis group and the non-septic SIRS group (8.4 [7.5-32.2] vs. 7.8 [1.9-17.5] ng/l; P = 0.67). On the other hand, we found that BPW was significantly higher in the sepsis group compared to the non-septic SIRS group (0.57 [0.54-0.78] vs. 0.19 [0.14-0.29] %T/s; P < 0.01). We found that a BPW threshold value of 0.465%T/s was able to discriminate between sepsis and non-septic SIRS groups with a sensitivity of 100% and a specificity of 93% (area under the curve: 0.948 +/- 0.039; P < 0.01). Applying the previously published threshold of 0.25%T/s, we found a sensitivity of 100% and a specificity of 72% to discriminate between these two groups. Neither C-reactive protein (CRP) nor PCT had significant predictive value (area under the curve for CRP was 0.659 +/- 0.142; P = 0.26 and area under the curve for PCT was 0.704 +/- 0.133; P = 0.15).
Conclusions: BPW has potential clinical applications for sepsis diagnosis in the postoperative period following cardiac surgery under CPB.
Figures
References
-
- Aouifi A, Piriou V, Blanc P, Bouvier H, Bastien O, Chiari P, Rousson R, Evans R, Lehot JJ. Effect of cardiopulmonary bypass on serum procalcitonin and C-reactive protein concentrations. Br J Anaesth. 1999;83:602–607. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
