

Cystic Fibrosis Foundation practice guidelines for the management of infants with cystic fibrosis transmembrane conductance regulator-related metabolic syndrome during the first two years of life and beyond
- PMID: 19914443
- PMCID: PMC6326077
- DOI: 10.1016/j.jpeds.2009.09.003
Cystic Fibrosis Foundation practice guidelines for the management of infants with cystic fibrosis transmembrane conductance regulator-related metabolic syndrome during the first two years of life and beyond
Abstract
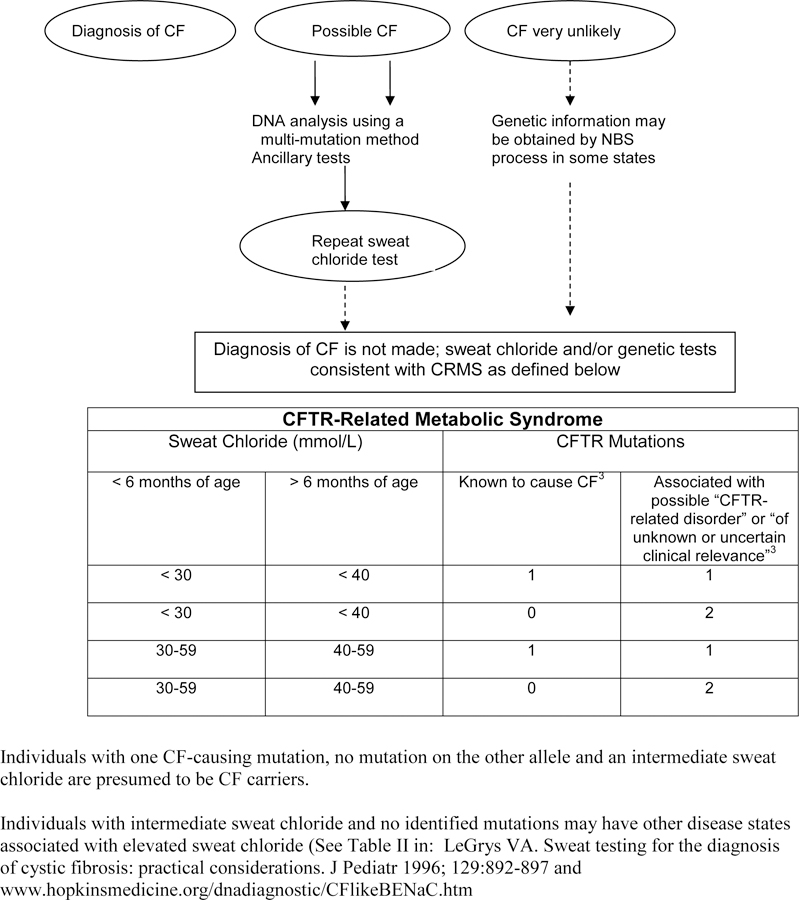
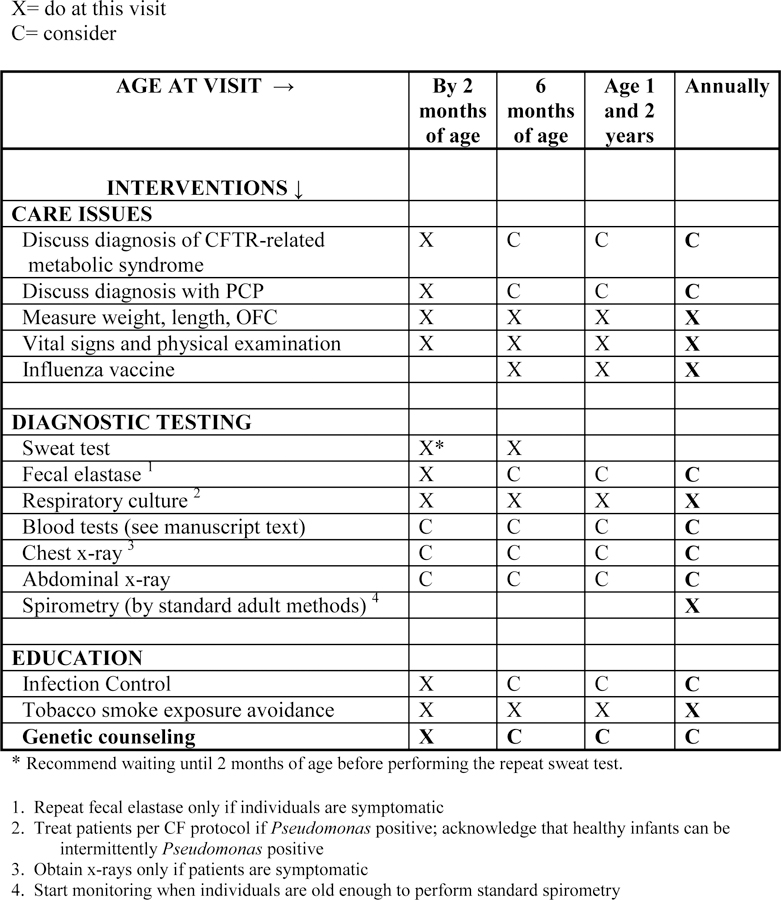
Through early detection, newborn screening (NBS)(1) for cystic fibrosis (CF) offers the opportunity for early intervention and improved outcomes. NBS programs screen for hypertrypsinogenemia, and most also identify mutations in the CF transmembrane conductance regulator (CFTR) gene. Individuals identified by NBS are diagnosed with CF if they have an elevated sweat chloride level or if they have inherited 2 disease-causing mutations in the CFTR gene. Mutations in the CFTR gene can cause CF, but not all CFTR mutations are disease-causing. The term CFTR-related metabolic syndrome (CRMS) is proposed to describe infants identified by hypertrypsinogenemia on NBS who have sweat chloride values <60 mmol/L and up to 2 CFTR mutations, at least 1 of which is not clearly categorized as a "CF-causing mutation," thus they do not meet CF Foundation guidelines for the diagnosis of CF. With what is now near-universal CF NBS in the United States, an increasing number of infants with CRMS are being identified. Given our inadequate knowledge of the natural history of CRMS, standards for diagnosis, monitoring, and treatment are absent. This document aims to help guide the monitoring and care of individuals with CRMS while our knowledge base on appropriate management evolves.
Figures
References
-
- Miller J, Petrie J. Development of practice guidelines. Lancet 2000;355(9198):82- - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
