

Issues regarding improving the impact of antiangiogenic drugs for the treatment of breast cancer
- PMID: 19914541
- PMCID: PMC4540343
- DOI: 10.1016/S0960-9776(09)70271-1
Issues regarding improving the impact of antiangiogenic drugs for the treatment of breast cancer
Abstract
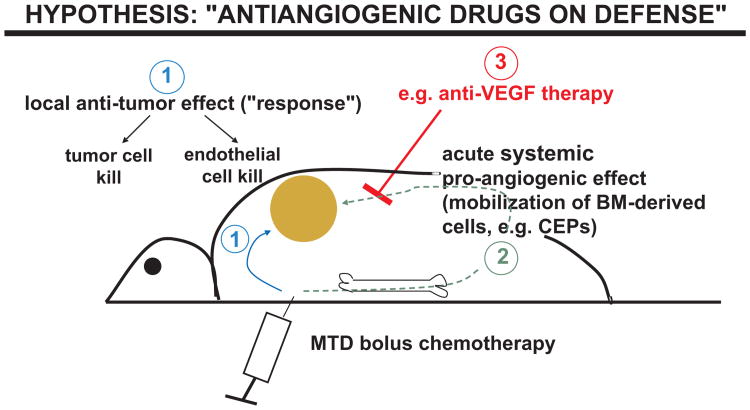
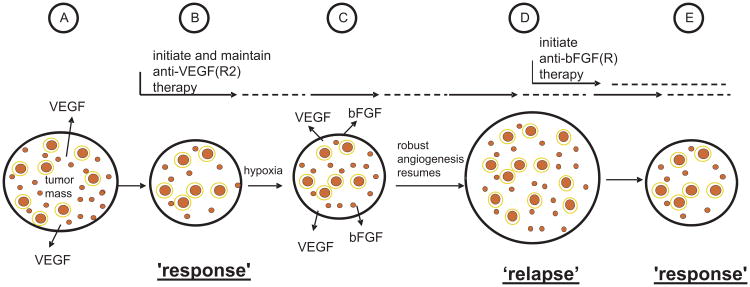
One of the major recent clinical advances in cancer treatment is the use of antiangiogenic drugs such as bevacizumab, sorafenib, and sunitinib. Bevacizumab, the monoclonal anti-VEGF antibody, has been approved for the first line treatment of metastatic breast cancer (MBC) when combined with taxane. However, the clinical benefits are modest; despite a doubling of response rates and significant prolongation of progression free survival times, no increase in overall survival is attained. This review summarizes some of the possibilities to account for this discrepant result. These include rapid development of acquired drug resistance due to the redundancy of proangiogenic growth factors, acceleration of tumor growth after antiangiogenic drug treatments are stopped, and increases in tumor cell malignant aggressiveness driven by mechanisms such as increased tumor hypoxia. Some possible strategies to improve the benefits of antiangiogenic drug therapy are discussed such as prolonging the treatment beyond tumor progression, combination with other therapeutic modalities, e.g. long term ('maintenance') low-dose metronomic chemotherapy or additional targeted/biologic drugs, e.g. trastuzumab.
Figures
References
-
- Kerbel RS. Antiangiogenic therapy: a universal chemosensitization strategy for cancer? Science. 2006;312:1171–5. - PubMed
-
- Chan A. Antiangiogenic therapy for metastatic breast cancer: current status and future directions. Drugs. 2009;69:167–81. - PubMed
-
- Miller K, Wang M, Gralow J, Dickler M, Cobleigh M, Perez EA, et al. Paclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancer. N Engl J Med. 2007;357:2666–76. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
