

Updating the profile of C-terminal MECP2 deletions in Rett syndrome
- PMID: 19914908
- PMCID: PMC3913726
- DOI: 10.1136/jmg.2009.072553
Updating the profile of C-terminal MECP2 deletions in Rett syndrome
Abstract
Objectives: This study aimed to compare the phenotype of Rett syndrome cases with C-terminal deletions to that of cases with different MECP2 mutations and to examine the phenotypic variation within C-terminal deletions.
Methods: Cases were selected from InterRett, an international database and from the population-based Australian Rett Syndrome Database. Cases (n=832) were included if they had a pathogenic MECP2 mutation in which the nature of the amino acid change was known. Three severity scale systems were used, and individual aspects of the phenotype were also compared.
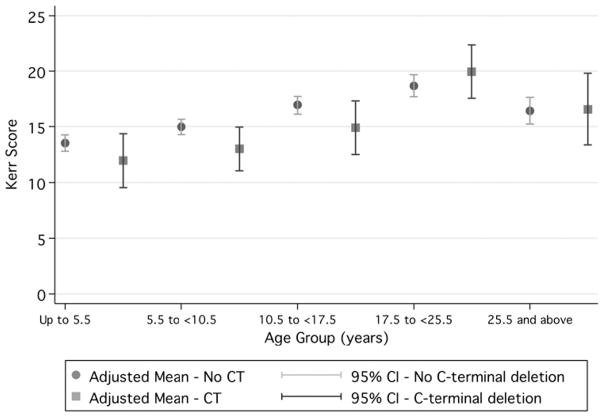
Results: Lower severity was associated with C-terminal deletions (n=79) compared to all other MECP2 mutations (e.g. Pineda scale C-terminals mean 15.0 (95% CI 14.0-16.0) vs 16.2 (15.9-16.5). Cases with C-terminal deletions were more likely to have a normal head circumference (odds ratio 3.22, 95% CI 1.53 - 6.79) and weight (odds ratio 2.97, 95% CI 1.25-5.76). Onset of stereotypies tended to be later (median age 2.5 years vs 2 years, p<0.001 from survival analysis), and age of learning to walk tended to be earlier (median age 1.6 years vs 2 years, p=0.002 from survival analysis). Those with C-terminal deletions occurring later in the region had lower average severity scores than those occurring earlier in the region.
Conclusion: In terms of overall severity C-terminal deletion cases would appear to be in the middle of the range. In terms of individual aspects of phenotype growth and ability to ambulate appear to be particular strengths. By pooling data internationally this study has achieved the case numbers to provide a phenotypic profile of C-terminal deletions in Rett syndrome.
Conflict of interest statement
Figures

References
-
- Hagberg B, Hanefeld F, Percy A, Skjeldal O. An update on clinically applicable diagnostic criteria in Rett syndrome. Comments to Rett Syndrome Clinical Criteria Consensus Panel Satellite to European Paediatric Neurology Society Meeting, Baden Baden, Germany, 11 September 2001. Europ J Paediatr Neurol. 2002;6:293–7. - PubMed
-
- Amir RE, Van den Veyver IB, Wan M, Tran CQ, Francke U, Zoghbi HY. Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat Genet. 1999;23:185–8. - PubMed
-
- Bebbington A, Leonard H, Ben Zeev B, et al. Investigating genotype–phenotype relationships in Rett syndrome using an international dataset. Neurology. 2008;70:868–75. - PubMed
-
- Renieri A. Diagnostic criteria for the zappella variant. Brain Dev. 2009;31:208–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical