

Immune profile and mitotic index of metastatic melanoma lesions enhance clinical staging in predicting patient survival
- PMID: 19915147
- PMCID: PMC2787158
- DOI: 10.1073/pnas.0905139106
Immune profile and mitotic index of metastatic melanoma lesions enhance clinical staging in predicting patient survival
Abstract
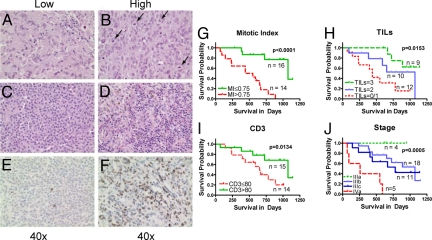
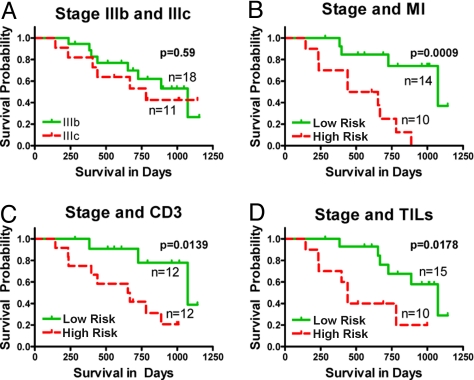
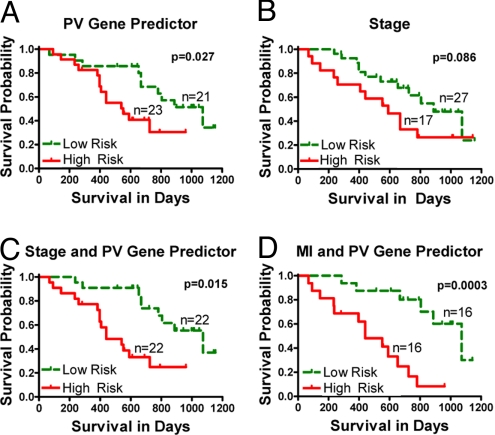
Although remission rates for metastatic melanoma are generally very poor, some patients can survive for prolonged periods following metastasis. We used gene expression profiling, mitotic index (MI), and quantification of tumor infiltrating leukocytes (TILs) and CD3+ cells in metastatic lesions to search for a molecular basis for this observation and to develop improved methods for predicting patient survival. We identified a group of 266 genes associated with postrecurrence survival. Genes positively associated with survival were predominantly immune response related (e.g., ICOS, CD3d, ZAP70, TRAT1, TARP, GZMK, LCK, CD2, CXCL13, CCL19, CCR7, VCAM1) while genes negatively associated with survival were cell proliferation related (e.g., PDE4D, CDK2, GREF1, NUSAP1, SPC24). Furthermore, any of the 4 parameters (prevalidated gene expression signature, TILs, CD3, and in particular MI) improved the ability of Tumor, Node, Metastasis (TNM) staging to predict postrecurrence survival; MI was the most significant contributor (HR = 2.13, P = 0.0008). An immune response gene expression signature and presence of TILs and CD3+ cells signify immune surveillance as a mechanism for prolonged survival in these patients and indicate improved patient subcategorization beyond current TNM staging.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Comment in
-
Tumor-infiltrating lymphocytes and mitotic index in metastatic melanoma as predictors of patient survival.Proc Natl Acad Sci U S A. 2010 Mar 30;107(13):E46; author reply E47. doi: 10.1073/pnas.0914657107. Epub 2010 Mar 22. Proc Natl Acad Sci U S A. 2010. PMID: 20308534 Free PMC article. No abstract available.
References
-
- Gray-Schopfer V, Wellbrock C, Marais R. Melanoma biology and new targeted therapy. Nature. 2007;445:851–857. - PubMed
-
- Thompson JF, Scolyer RA, Kefford RF. Cutaneous melanoma. Lancet. 2005;365:687–701. - PubMed
-
- Fecher LA, Cummings SD, Keefe MJ, Alani RM. Toward a molecular classification of melanoma. J Clin Oncol. 2007;25:1606–1620. - PubMed
-
- Balch CM, Soong SJ. Predicting outcomes in metastatic melanoma. J Clin Oncol. 2008;26:168–169. - PubMed
-
- Golub TR, et al. Molecular classification of cancer: Class discovery and class prediction by gene expression monitoring. Science. 1999;286:531–537. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
