

Dosimetry during intramedullary nailing of the tibia
- PMID: 19916691
- PMCID: PMC2823322
- DOI: 10.3109/17453670903350057
Dosimetry during intramedullary nailing of the tibia
Abstract
Background: Intramedullary nailing under fluoroscopic guidance is a common operation. We studied the intraoperative radiation dose received by both the patient and the personnel.
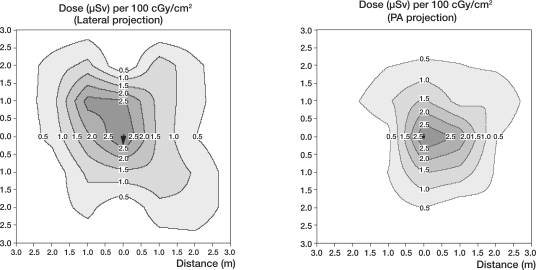
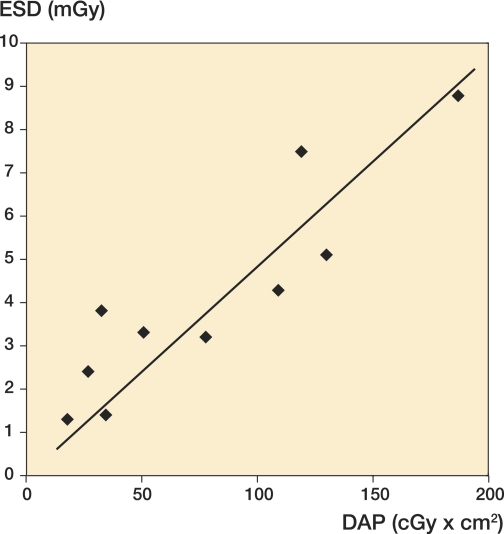
Patients and methods: 25 intramedullary nailing procedures of the tibia were studied. All patients suffered from tibial fractures and were treated using the Grosse-Kempf intramedullary nail, with free-hand technique for fixation of the distal screws, under fluoroscopic guidance. The exposure, at selected positions, was recorded using an ion chamber, while the dose area product (DAP) was measured with a DAP meter, attached to the tube head. Thermoluminescent dosimeters (TLDs) were used to derive the occupational dose to the personnel, and also to monitor the surface dose on the gonads of some of the patients.
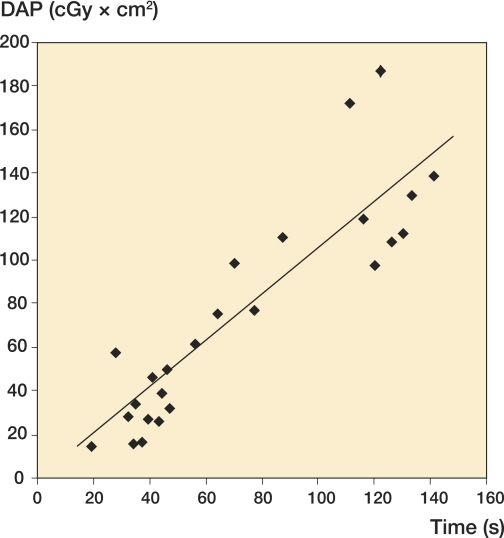
Results: The mean operation time was 101 (48-240) min, with a mean fluoroscopic time of 72 seconds and a mean DAP value of 75 cGy x cm(2). The surface dose to the gonads of the patients was less than 8.8 mGy during any procedure, and thus cannot be considered to be a contraindication for the use of this technique. Occupational dose differed substantially between members of the operating personnel, the maximum dose recorded being to the operator of the fluoroscopic equipment (0.11 mSv).
Interpretation: Our findings underscore the care required by the primary operator not to exceed the dose constraint of 10 mSv per year. The rest of the operating personnel, although they do not receive very high doses, should focus on the dose optimization of the technique.
Figures



References
-
- Blattert TR, Fill UA, Kunz E, Panzer W, Weckbach A, Regulla DF. Skill dependence of radiation exposure for the orthopaedic surgeon during interlocking nailing of long-bone shaft fractures: A clinical study. Arch Orthop Trauma Surg. 2004;124((10)):659–64. - PubMed
-
- Conference of Radiation Control Program Directors (CRCPD) Quality control recommendations for diagnostic radiography. Volume 3, radiographic or fluoroscopic machines. CRCPD Publication 01-6, Frankfort, Kentucky, 2001
-
- Crawley MT, Rogers AT. Dose-area product measurements in a range of common orthopaedic procedures and their possible use in establishing local diagnostic reference levels. Br J Radiol. 2000;73:740–4. - PubMed
-
- Fitousi NT, Efstathopoulos EP, Delis HB, Kottou S, Kelekis AD, Panayiotakis GS. Patient and staff dosimetry in vertebroplasty. Spine. 2006;31((23)):E884–E889. - PubMed
-
- Hafez MA, Smith RM, Matthews SJ, Kalap G, Sherman K. Radiation exposure to the hands of orthopaedic surgeons: Are we underestimating the risk? Arch Orthop Trauma Surg. 2005;125((5)):330–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical