

A subset of patients destined to develop spontaneous preterm labor has an abnormal angiogenic/anti-angiogenic profile in maternal plasma: evidence in support of pathophysiologic heterogeneity of preterm labor derived from a longitudinal study
- PMID: 19916710
- PMCID: PMC3437777
- DOI: 10.3109/14767050902994838
A subset of patients destined to develop spontaneous preterm labor has an abnormal angiogenic/anti-angiogenic profile in maternal plasma: evidence in support of pathophysiologic heterogeneity of preterm labor derived from a longitudinal study
Abstract
Objective: An imbalance between angiogenic and anti-angiogenic factors in maternal blood has been observed in several obstetrical syndromes including preeclampsia, pregnancies with fetal growth restriction and fetal death. Vascular lesions have been identified in a subset of patients with spontaneous preterm labor (PTL). It is possible that PTL may be one of the manifestations of an anti-angiogenic state. The aim of this study was to determine if patients prior to the clinical diagnosis of PTL leading to preterm delivery had plasma concentrations of angiogenic and anti-angiogenic factors different from normal pregnant women.
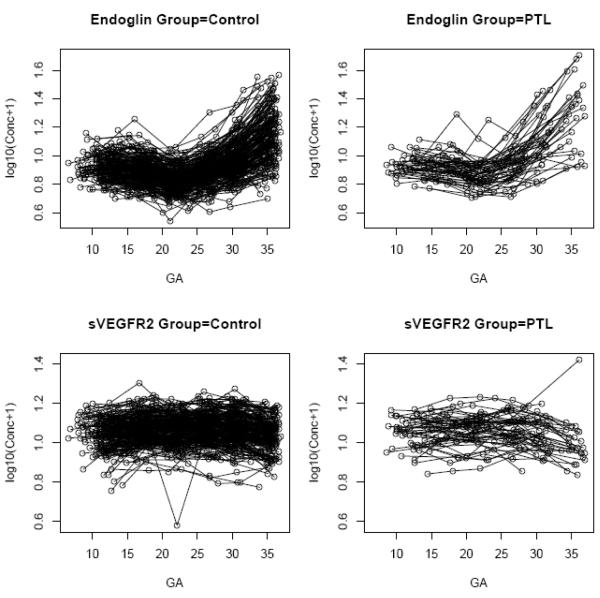
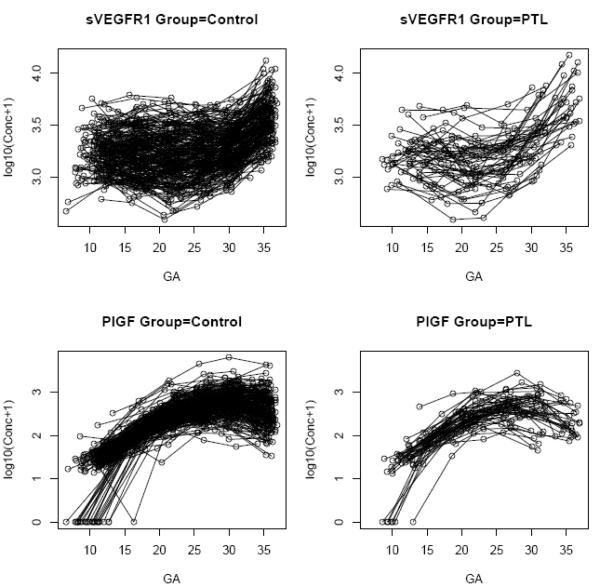
Study design: This longitudinal nested case-control study included normal pregnant women (n = 208) and patients with PTL leading to preterm delivery (n = 52). Maternal blood samples were collected at 6 gestational age intervals from 6 to 36.9 weeks of gestation. The end point (time of diagnosis) of the study, 'True PTL', was defined as patients presenting with PTL and delivered within 1 day. Plasma concentrations of sVEGFR-1, sVEGFR-2, sEng and PlGF were determined by ELISA. Analysis was performed with both cross-sectional and longitudinal (mixed effects model) approaches.
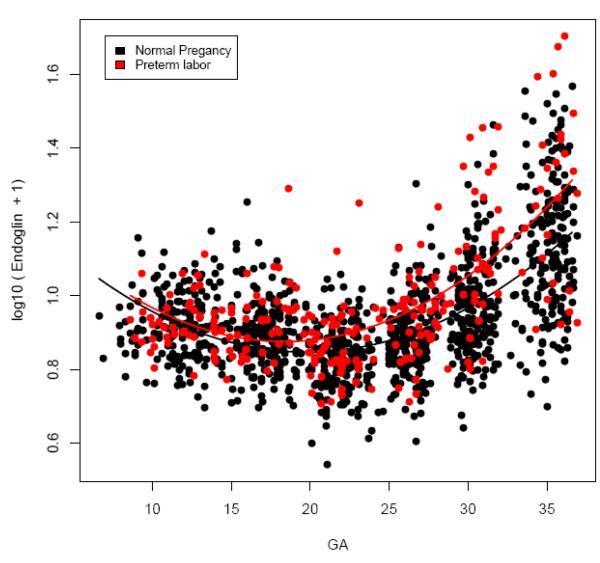
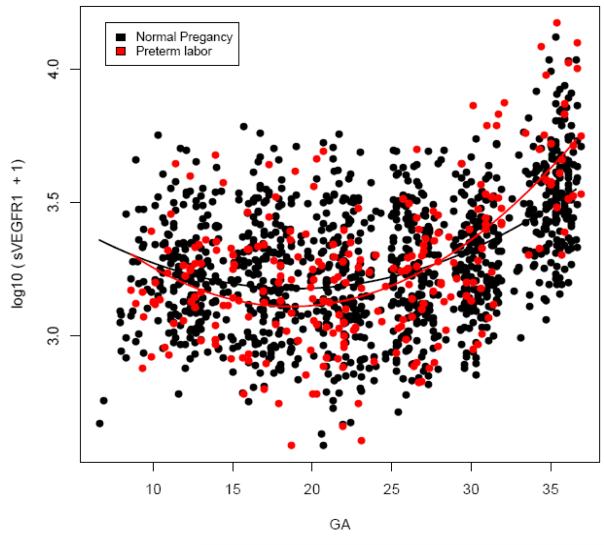
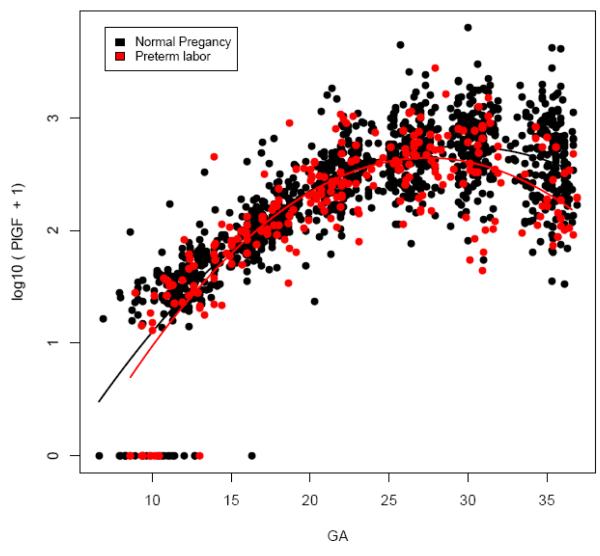
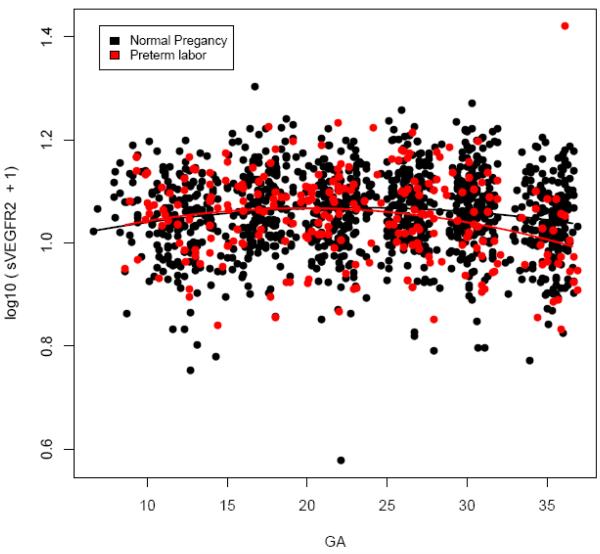
Results: (1) Plasma sEng concentration in patients destined to develop PTL was higher than that in normal pregnant women from 15-20 weeks of gestation. The difference became statistical significant at 28 weeks of gestation, or approximately 5-10 weeks prior to the diagnosis of 'true PTL'. (2) Backward analysis suggests that plasma concentrations of PlGF and sVEGFR-2 were lower, and those of sVEGFR-1 were higher in patients with PTL than in normal pregnant women less than 5 weeks prior to the diagnosis of 'true PTL'; and (3) Plasma concentrations of sEng and sVEGFR-1 were higher and those of PlGF and sVEGFR-2 were lower in patients diagnosed with PTL and delivery within 1 day than in normal pregnant women who delivered at term.
Conclusion: The changes in sEng are demonstrable several weeks prior to the onset of preterm parturition. In contrast, the changes in the other angiogenic proteins are present close to the onset of PTL and delivery. This observation supports the view that an imbalance of angiogenic factors participates in the pathophysiology of spontaneous preterm parturition.
Figures
Similar articles
-
An imbalance between angiogenic and anti-angiogenic factors precedes fetal death in a subset of patients: results of a longitudinal study.J Matern Fetal Neonatal Med. 2010 Dec;23(12):1384-99. doi: 10.3109/14767051003681121. Epub 2010 May 12. J Matern Fetal Neonatal Med. 2010. PMID: 20459337 Free PMC article.
-
A longitudinal study of angiogenic (placental growth factor) and anti-angiogenic (soluble endoglin and soluble vascular endothelial growth factor receptor-1) factors in normal pregnancy and patients destined to develop preeclampsia and deliver a small for gestational age neonate.J Matern Fetal Neonatal Med. 2008 Jan;21(1):9-23. doi: 10.1080/14767050701830480. J Matern Fetal Neonatal Med. 2008. PMID: 18175241 Free PMC article.
-
The use of angiogenic biomarkers in maternal blood to identify which SGA fetuses will require a preterm delivery and mothers who will develop pre-eclampsia.J Matern Fetal Neonatal Med. 2016;29(8):1214-28. doi: 10.3109/14767058.2015.1048431. J Matern Fetal Neonatal Med. 2016. PMID: 26303962 Free PMC article.
-
Unexplained fetal death: another anti-angiogenic state.J Matern Fetal Neonatal Med. 2007 Jul;20(7):495-507. doi: 10.1080/14767050701413022. J Matern Fetal Neonatal Med. 2007. PMID: 17674262 Free PMC article.
-
The preterm parturition syndrome.BJOG. 2006 Dec;113 Suppl 3(Suppl 3):17-42. doi: 10.1111/j.1471-0528.2006.01120.x. BJOG. 2006. PMID: 17206962 Free PMC article. Review.
Cited by
-
On the pitfalls of adjusting for gestational age at birth.Am J Epidemiol. 2011 Nov 1;174(9):1062-8. doi: 10.1093/aje/kwr230. Epub 2011 Sep 26. Am J Epidemiol. 2011. PMID: 21946386 Free PMC article.
-
The "Great Obstetrical Syndromes" are associated with disorders of deep placentation.Am J Obstet Gynecol. 2011 Mar;204(3):193-201. doi: 10.1016/j.ajog.2010.08.009. Epub 2010 Nov 20. Am J Obstet Gynecol. 2011. PMID: 21094932 Free PMC article. Review.
-
Low dose aspirin in the prevention of recurrent spontaneous preterm labour - the APRIL study: a multicenter randomized placebo controlled trial.BMC Pregnancy Childbirth. 2017 Jul 14;17(1):223. doi: 10.1186/s12884-017-1338-0. BMC Pregnancy Childbirth. 2017. PMID: 28705190 Free PMC article. Clinical Trial.
-
Spontaneous Preterm Birth: a Fetal-Maternal Metabolic Imbalance.Matern Fetal Med. 2023 Oct 20;5(4):223-228. doi: 10.1097/FM9.0000000000000205. eCollection 2023 Oct. Matern Fetal Med. 2023. PMID: 40406555 Free PMC article.
-
Mid-pregnancy levels of angiogenic markers as indicators of pathways to preterm delivery.J Matern Fetal Neonatal Med. 2012 Jul;25(7):1135-41. doi: 10.3109/14767058.2011.625458. Epub 2011 Oct 24. J Matern Fetal Neonatal Med. 2012. PMID: 21939291 Free PMC article.
References
-
- Iams JD, Romero R, Culhane JF, Goldenberg RL. Primary, secondary, and tertiary interventions to reduce the morbidity and mortality of preterm birth. Lancet. 2008;371:164–175. - PubMed
-
- Mathews TJ, MacDorman MF. Infant mortality statistics from the 2005 period linked birth/infant death data set. Natl.Vital Stat.Rep. 2008;57:1–32. - PubMed
-
- Romero R, Sirtori M, Oyarzun E, Avila C, Mazor M, Callahan R, Sabo V, Athanassiadis AP, Hobbins JC. Infection and labor. V. Prevalence, microbiology, and clinical significance of intraamniotic infection in women with preterm labor and intact membranes. Am J Obstet Gynecol. 1989;161:817–824. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources