

Functional measurements based on feature tracking of cine magnetic resonance images identify left ventricular segments with myocardial scar
- PMID: 19917130
- PMCID: PMC2785780
- DOI: 10.1186/1476-7120-7-53
Functional measurements based on feature tracking of cine magnetic resonance images identify left ventricular segments with myocardial scar
Abstract
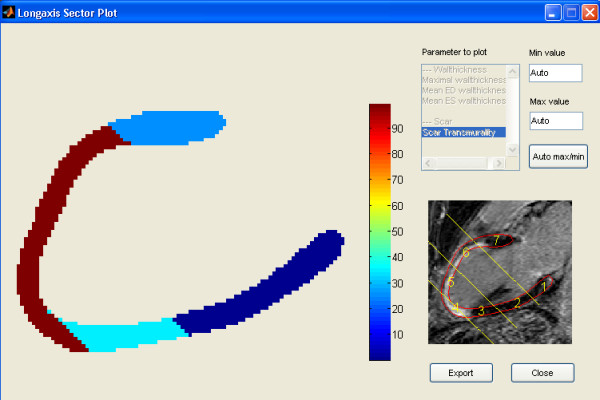
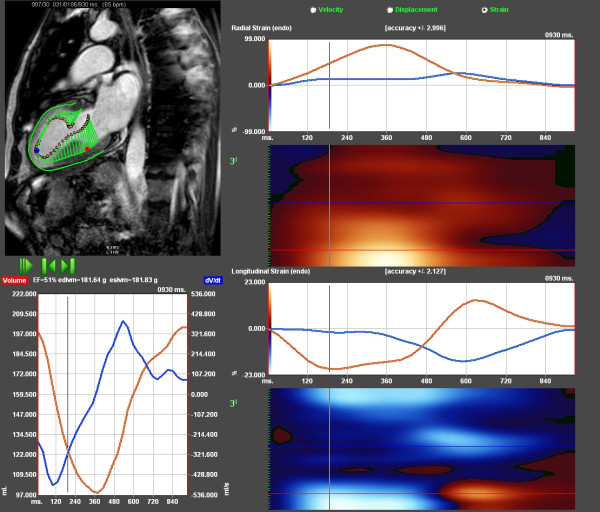
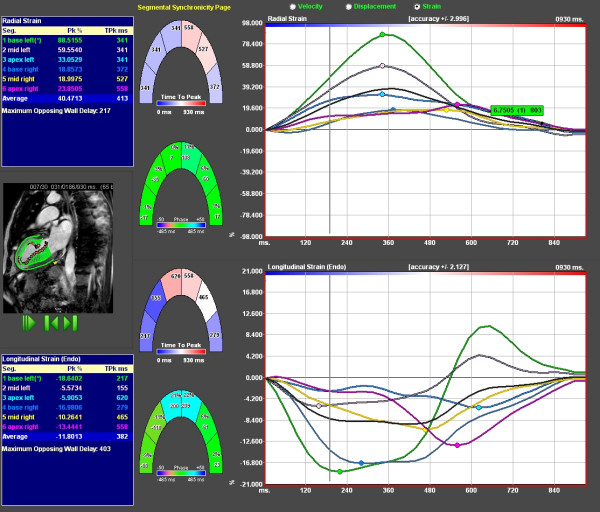
Background: The aim of the study was to perform a feature tracking analysis on cine magnetic resonance (MR) images to elucidate if functional measurements of the motion of the left ventricular wall may detect scar defined with gadolinium enhanced MR.Myocardial contraction can be measured in terms of the velocity, displacement and local deformation (strain) of a particular myocardial segment. Contraction of the myocardial wall will be reduced in the presence of scar and as a consequence of reduced myocardial blood flow.
Methods: Thirty patients (3 women and 27 men) were selected based on the presence or absence of extensive scar in the anteroseptal area of the left ventricle. The patients were investigated in stable clinical condition, 4-8 weeks post ST-elevation myocardial infarction treated with percutaneous coronary intervention. Seventeen had a scar area >75% in at least one anteroseptal segment (scar) and thirteen had scar area <1% (non-scar). Velocity, displacement and strain were calculated in the longitudinal direction, tangential to the endocardial outline, and in the radial direction, perpendicular to the tangent.
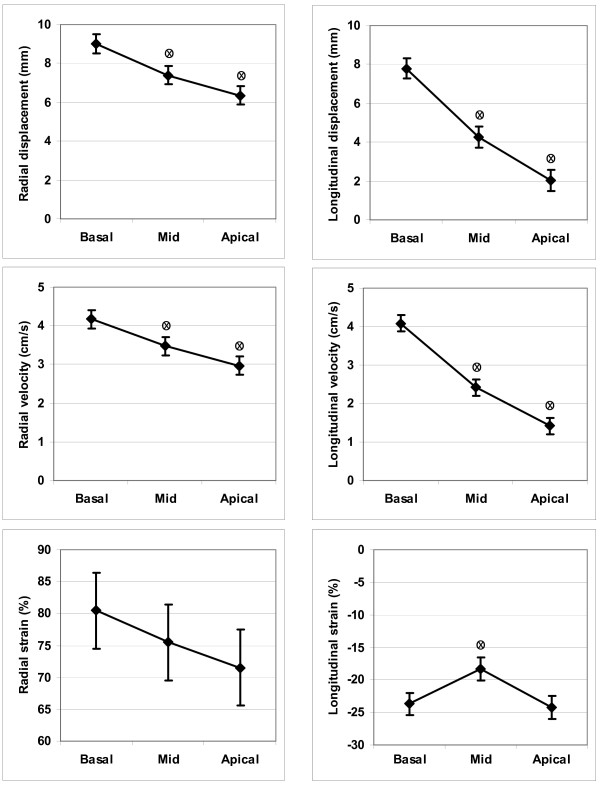
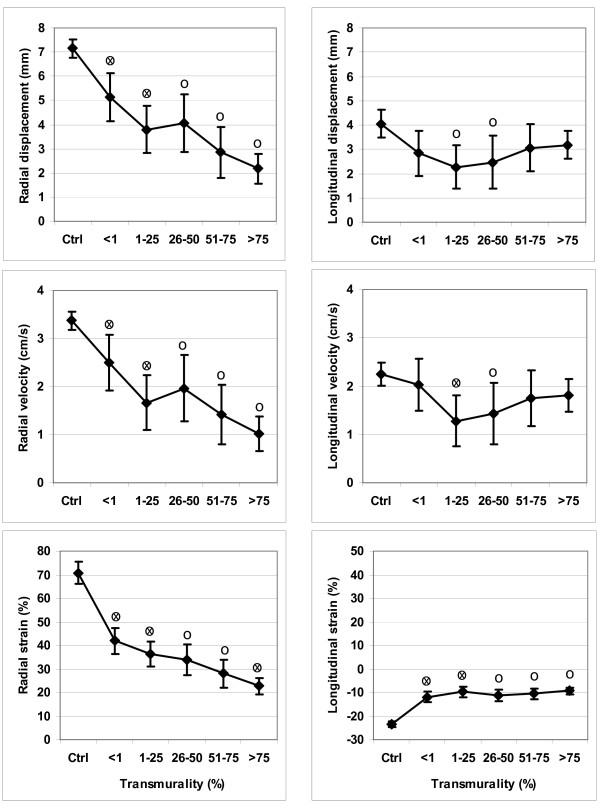
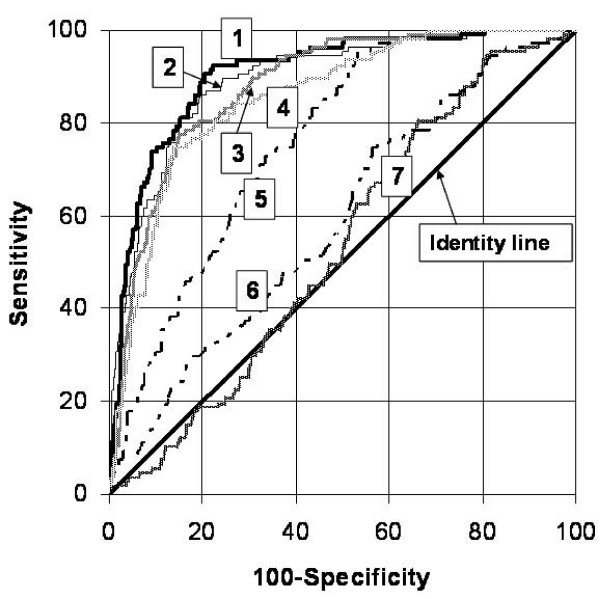
Results: In the scar patients, segments with scar showed lower functional measurements than remote segments. Radial measurements of velocity, displacement and strain performed better in terms of receiver-operator-characteristic curves (ROC) than the corresponding longitudinal measurements. The best area-under-curve was for radial strain, 0.89, where a cut-off value of 38.8% had 80% sensitivity and 86% specificity for the detection of a segment with scar area >50%. As a percentage of the mean, intraobserver variability was 16-14-26% for radial measurements of displacement-velocity-strain and corresponding interobserver variability was 13-12-18%.
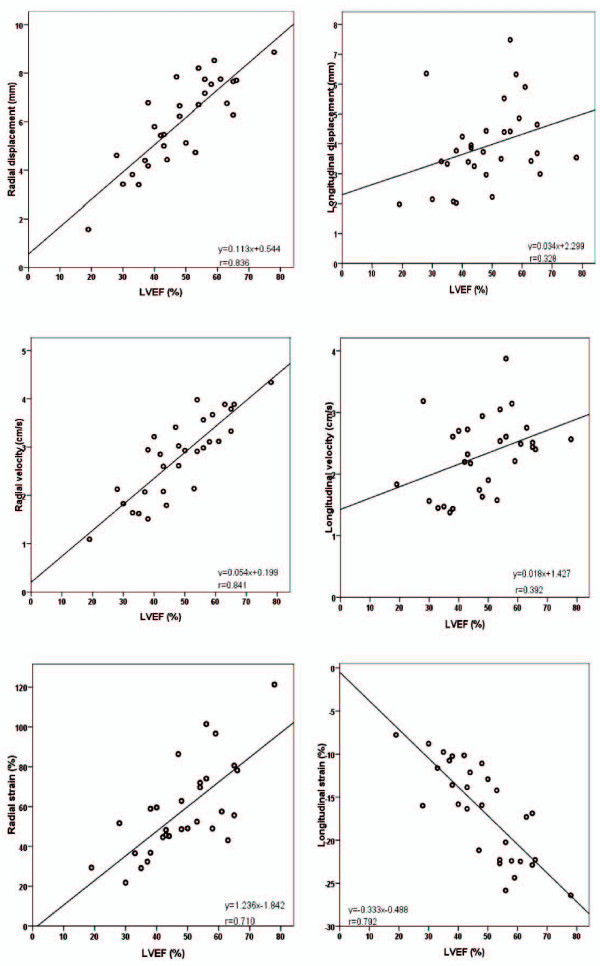
Conclusion: Feature tracking analysis of cine-MR displays velocity, displacement and strain in the radial and longitudinal direction and may be used for the detection of transmural scar. The accuracy and repeatability of the radial functional measurements is satisfactory and global measures agree.
Figures
References
-
- Hoffmann R, Lethen H, Marwick T, Arnese M, Fioretti P, Pingitore A, Picano E, Buck T, Erbel R, Flachskampf FA. Analysis of interinstitutional observer agreement in interpretation of dobutamine stress echocardiograms. J Am Coll Cardiol. 1996;27(2):330–336. doi: 10.1016/0735-1097(95)00483-1. - DOI - PubMed
-
- Madler CF, Payne N, Wilkenshoff U, Cohen A, Derumeaux GA, Pierard LA, Engvall J, Brodin LA, Sutherland GR, Fraser AG. Non-invasive diagnosis of coronary artery disease by quantitative stress echocardiography: optimal diagnostic models using off-line tissue Doppler in the MYDISE study. Eur Heart J. 2003;24(17):1584–1594. doi: 10.1016/S0195-668X(03)00099-X. - DOI - PubMed
-
- Amundsen BH, Crosby J, Steen PA, Torp H, Slordahl SA, Stoylen A. Regional myocardial long-axis strain and strain rate measured by different tissue Doppler and speckle tracking echocardiography methods: a comparison with tagged magnetic resonance imaging. Eur J Echocardiogr. 2008. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
