

Induction chemotherapy and cetuximab for locally advanced squamous cell carcinoma of the head and neck: results from a phase II prospective trial
- PMID: 19917840
- PMCID: PMC2799235
- DOI: 10.1200/JCO.2009.23.0425
Induction chemotherapy and cetuximab for locally advanced squamous cell carcinoma of the head and neck: results from a phase II prospective trial
Abstract
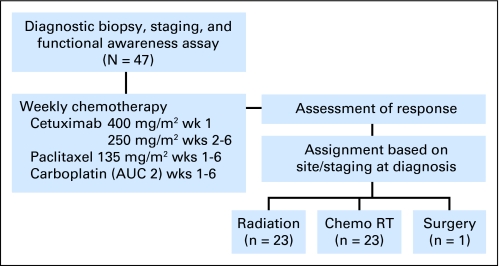
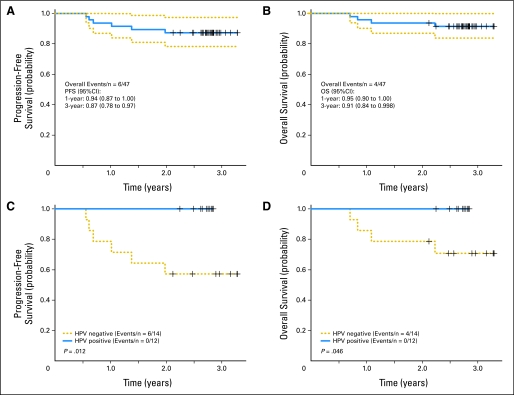
PURPOSE To determine the potential efficacy of combining cetuximab with chemotherapy in patients with advanced nodal disease, we conducted a phase II trial with induction chemotherapy (ICT) consisting of six weekly cycles of paclitaxel 135 mg/m(2) and carboplatin (area under the curve = 2) with cetuximab 400 mg/m(2) in week 1 and then 250 mg/m(2) (PCC). PATIENTS AND METHODS Forty-seven previously untreated patients (41 with oropharynx primaries; 33 men, 14 women; median age, 53 years; performance status of 0 or 1) with squamous cell carcinoma of the head and neck (SCCHN; T1-4, N2b/c/3) were treated and evaluated for clinical and radiographic response. After ICT, patients underwent risk-based local therapy, which consisted of either radiation, concomitant chemoradiotherapy, or surgery, based on tumor stage and site at diagnosis. Results After induction PCC, nine patients (19%) achieved a complete response, and 36 patients (77%) achieved a partial response. The most common grade 3 or 4 toxicity was skin rash (45%), followed by neutropenia (21%) without fever. At a median follow-up time of 33 months, locoregional or systemic disease progression was observed in six patients. The 3-year progression-free survival (PFS) and overall survival (OS) rates were 87% (95% CI, 78% to 97%) and 91% (95% CI, 84% to 99%), respectively. Human papillomavirus (HPV) 16, found in 12 (46%) of 26 biopsies, was associated with improved PFS (P = .012) and OS (P = .046). CONCLUSION ICT with weekly PCC followed by risk-based local therapy seems to be feasible, effective, and well tolerated. PFS is promising, and this sequential treatment strategy should be further investigated. Patients with HPV-positive tumors have an excellent prognosis.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
- J Clin Oncol. 28:1.
References
-
- Adelstein DJ, Leblanc M. Does induction chemotherapy have a role in the management of locoregionally advanced squamous cell head and neck cancer? J Clin Oncol. 2006;24:2624–2628. - PubMed
-
- Brockstein B, Haraf DJ, Rademaker AW, et al. Patterns of failure, prognostic factors and survival in locoregionally advanced head and neck cancer treated with concomitant chemoradiotherapy: A 9-year, 337-patient, multi-institutional experience. Ann Oncol. 2004;15:1179–1186. - PubMed
-
- Garden AS. Where are the at-risk cervical nodes? Int J Radiat Oncol Biol Phys. 2004;58:1–2. - PubMed
-
- Garden AS, Asper JA, Morrison WH, et al. Is concurrent chemoradiation the treatment of choice for all patients with Stage III or IV head and neck carcinoma? Cancer. 2004;100:1171–1178. - PubMed
-
- Pignon JP, Bourhis J, Domenge C, et al. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: Three meta-analyses of updated individual data—Meta-Analysis of Chemotherapy on Head and Neck Cancer Collaborative Group. Lancet. 2000;355:949–955. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
