

Postprandial diabetic glucose tolerance is normalized by gastric bypass feeding as opposed to gastric feeding and is associated with exaggerated GLP-1 secretion: a case report
- PMID: 19918005
- PMCID: PMC2809286
- DOI: 10.2337/dc09-1374
Postprandial diabetic glucose tolerance is normalized by gastric bypass feeding as opposed to gastric feeding and is associated with exaggerated GLP-1 secretion: a case report
Abstract
Objective: To examine after gastric bypass the effect of peroral versus gastroduodenal feeding on glucose metabolism.
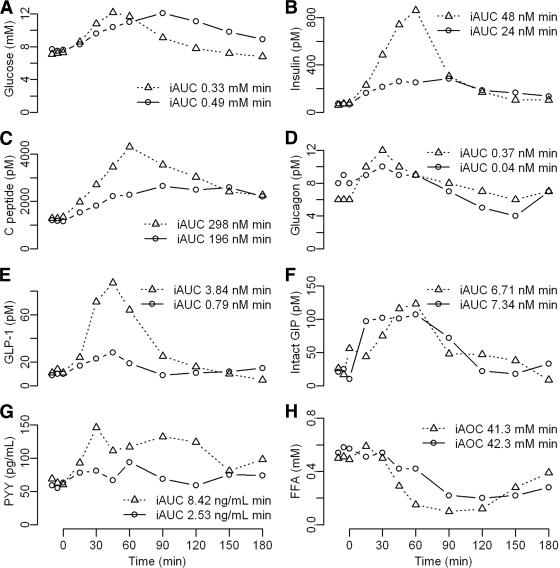
Research design and methods: A type 2 diabetic patient was examined on 2 consecutive days 5 weeks after gastric bypass. A standard liquid meal was given on the first day into the bypassed gastric remnant and on the second day perorally. Plasma glucose, insulin, C-peptide, glucagon, incretin hormones, peptide YY, and free fatty acids were measured.
Results: Peroral feeding reduced 2-h postprandial plasma glucose (7.8 vs. 11.1 mmol/l) and incremental area under the glucose curve (iAUC) (0.33 vs. 0.49 mmol . l(-1) . min(-1)) compared with gastroduodenal feeding. beta-Cell function (iAUC(Cpeptide/Glu)) was more than twofold improved during peroral feeding, and the glucagon-like peptide (GLP)-1 response increased nearly fivefold.
Conclusions: Improvement in postprandial glucose metabolism after gastric bypass is an immediate and direct consequence of the gastrointestinal rearrangement, associated with exaggerated GLP-1 release and independent of changes in insulin sensitivity, weight loss, and caloric restriction.
Figures
References
-
- Buchwald H, Avidor Y, Braunwald E, Jensen MD, Pories W, Fahrbach K, Schoelles K. Bariatric surgery: a systematic review and meta-analysis. JAMA 2004; 292: 1724– 1737 - PubMed
-
- Højberg PV, Vilsbøll T, Rabøl R, Knop FK, Bache M, Krarup T, Holst JJ, Madsbad S. Four weeks of near-normalisation of blood glucose improves the insulin response to glucagon-like peptide-1 and glucose-dependent insulinotropic polypeptide in patients with type 2 diabetes. Diabetologia 2009; 52: 199– 207 - PubMed
-
- Nauck M, Stöckmann F, Ebert R, Creutzfeldt W. Reduced incretin effect in type 2 (non-insulin-dependent) diabetes. Diabetologia 1986; 29: 46– 52 - PubMed
-
- Borg CM, le Roux CW, Ghatei MA, Bloom SR, Patel AG, Aylwin SJ. Progressive rise in gut hormone levels after Roux-en-Y gastric bypass suggests gut adaptation and explains altered satiety. Br J Surg 2006; 93: 210– 215 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
