

Genomic profiling of atypical meningiomas associates gain of 1q with poor clinical outcome
- PMID: 19918127
- PMCID: PMC2847373
- DOI: 10.1097/NEN.0b013e3181ba3952
Genomic profiling of atypical meningiomas associates gain of 1q with poor clinical outcome
Abstract
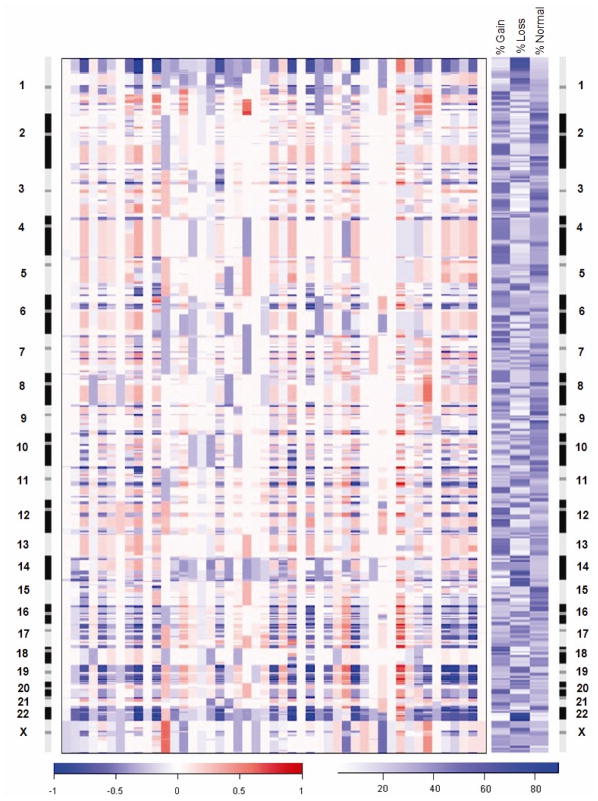
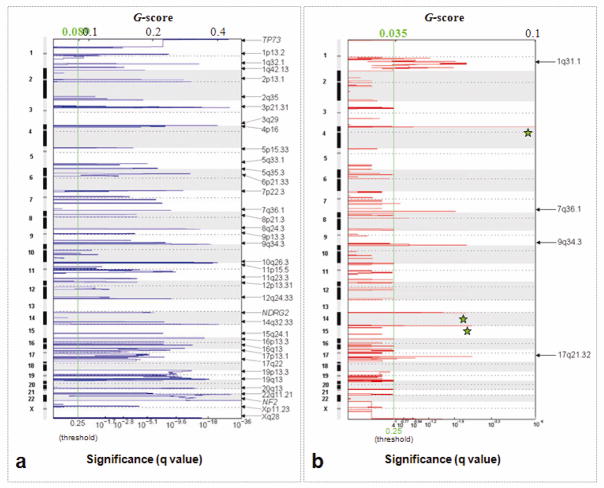
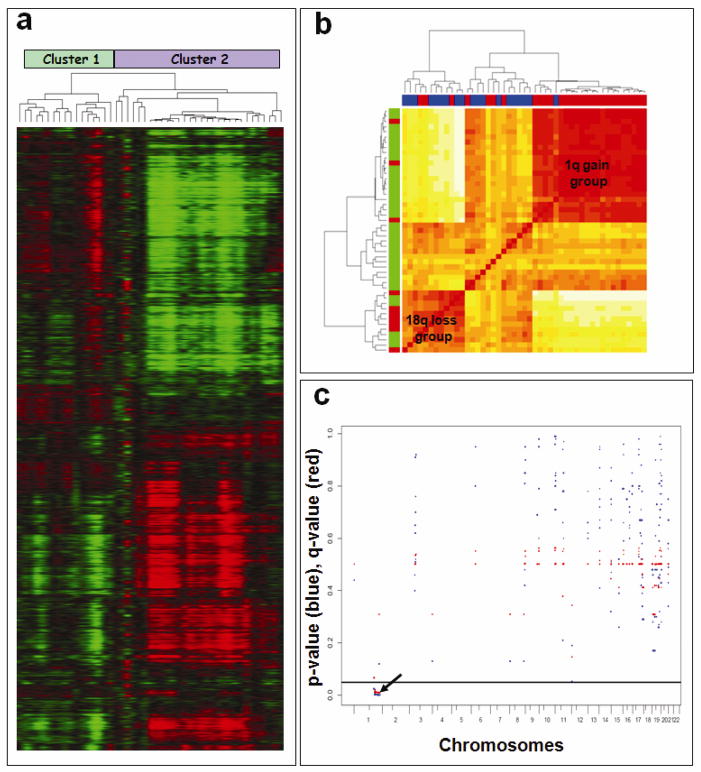
Atypical meningiomas exhibit heterogeneous clinical outcomes. It is unclear which atypical meningiomas require aggressive multimodality treatment with surgery and radiation therapy versus surgery alone to prevent recurrence. Detailed molecular-genetic characterization of these neoplasms is necessary to understand their pathogenesis and identify clinically relevant genetic markers. Oligonucleotide array comparative genomic hybridization was used to identify frequent genetic alterations in 47 primary atypical meningiomas resected at Massachusetts General Hospital between August 1987 and September 2006. Eighty-five percent of samples exhibited loss of 22q, including the neurofibromatosis type 2 gene. The second most frequent regions of loss were confined to the short arm of chromosome 1, particularly 1p33-p36.2 (70%) and 1p13.2 (64%). Other frequent regions of loss, detected in more than 50% of samples, included 14q, 10q, 8q, 7p, 21q, 19, 9q34, and 4p16. Frequent regions of gain were detected along 1q (59%), 17q (44%), 9q34 (30%), and 7q36 (26%). Univariate marker-by-marker analysis of all frequently identified copy number alterations showed potential correlation between gain of 1q and shorter progression-free survival. Given the heterogeneous treatment outcomes of atypical meningioma, investigation of large-scale and focal genomic alterations in multi-institutional efforts may help clarify molecular-genetic signatures of clinical use.
Figures
References
-
- Goyal LK, Suh JH, Mohan DS, Prayson RA, Lee J, Barnett GH. Local control and overall survival in atypical meningioma: a retrospective study. Int J Radiat Oncol Biol Phys. 2000;46:57–61. - PubMed
-
- Dziuk TW, Woo S, Butler EB, Thornby J, Grossman R, Dennis WS, Lu H, Carpenter LS, Chiu JK. Malignant meningioma: an indication for initial aggressive surgery and adjuvant radiotherapy. J Neurooncol. 1998;37:177–88. - PubMed
-
- Willis J, Smith C, Ironside JW, Erridge S, Whittle IR, Everington D. The accuracy of meningioma grading: a 10-year retrospective audit. Neuropathol Appl Neurobiol. 2005;31:141–9. - PubMed
-
- Palma L, Celli P, Franco C, Cervoni L, Cantore G. Long-term prognosis for atypical and malignant meningiomas: a study of 71 surgical cases. J Neurosurg. 1997;86:793–800. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
