

Comparing planning time, delivery time and plan quality for IMRT, RapidArc and Tomotherapy
- PMID: 19918236
- PMCID: PMC5720582
- DOI: 10.1120/jacmp.v10i4.3068
Comparing planning time, delivery time and plan quality for IMRT, RapidArc and Tomotherapy
Abstract
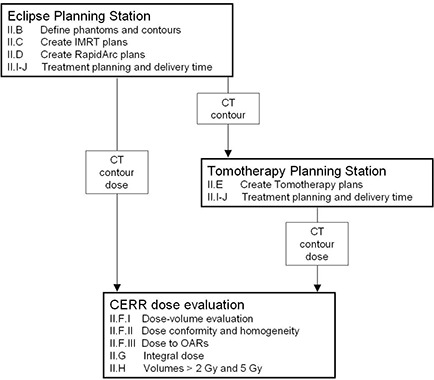
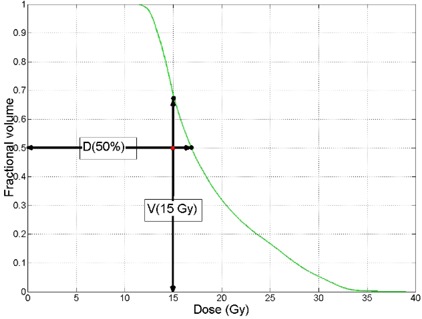
The purpose of this study is to examine plan quality, treatment planning time, and estimated treatment delivery time for 5- and 9-field sliding window IMRT, single and dual arc RapidArc, and tomotherapy. For four phantoms, 5- and 9-field IMRT, single and dual arc RapidArc and tomotherapy plans were created. Plans were evaluated based on the ability to meet dose-volume constraints, dose homogeneity index, radiation conformity index, planning time, estimated delivery time, integral dose, and volume receiving more than 2 and 5 Gy. For all of the phantoms, tomotherapy was able to meet the most optimization criteria during planning (50% for P1, 67% for P2, 0% for P3, and 50% for P4). RapidArc met less of the optimization criteria (25% for P1, 17% for P2, 0% for P3, and 0% for P4), while IMRT was never able to meet any of the constraints. In addition, tomotherapy plans were able to produce the most homogeneous dose. Tomotherapy plans had longer planning time, longer estimated treatment times, lower conformity index, and higher integral dose. Tomotherapy plans can produce plans of higher quality and have the capability to conform dose distributions better than IMRT or RapidArc in the axial plane, but exhibit increased dose superior and inferior to the target volume. RapidArc, however, is capable of producing better plans than IMRT for the test cases examined in this study.
Figures




References
-
- Yu CX, Amies CJ, Svatos M. Planning and delivery of intensity‐modulated radiation therapy. Med Phys. 2008;35(12):5233–41. - PubMed
-
- Ling CC, Burman C, Chui CS, et al. Conformal radiation treatment of prostate cancer using inversely‐planned intensity‐modulated photon beams produced with dynamic multileaf collimation. Int J Radiat Oncol Biol Phys. 1996;35(4):721–30. - PubMed
-
- Fraass BA, Kessler ML, McShan DL, et al. Optimization and clinical use of multisegment intensity‐modulated radiation therapy for high‐dose conformal therapy. Semin Radiat Oncol. 1999;9(1):60–77. - PubMed
-
- Intensity Modulated Radiation Therapy Collaborative Working Group. Intensity‐modulated radiotherapy: current status and issues of interest. Int J Radiat Oncol Biol Phys. 2001;51(4):880–914. - PubMed
-
- Veldeman L, Madani I, Hulstaert F, De Meerleer G, Mareel M, De Neve W. Evidence behind use of intensity‐modulated radiotherapy: a systematic review of comparative clinical studies. Lancet Oncol. 2008;9(4):367–75. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
