

Bone disease after renal transplantation
- PMID: 19918255
- PMCID: PMC4503388
- DOI: 10.1038/nrneph.2009.192
Bone disease after renal transplantation
Abstract
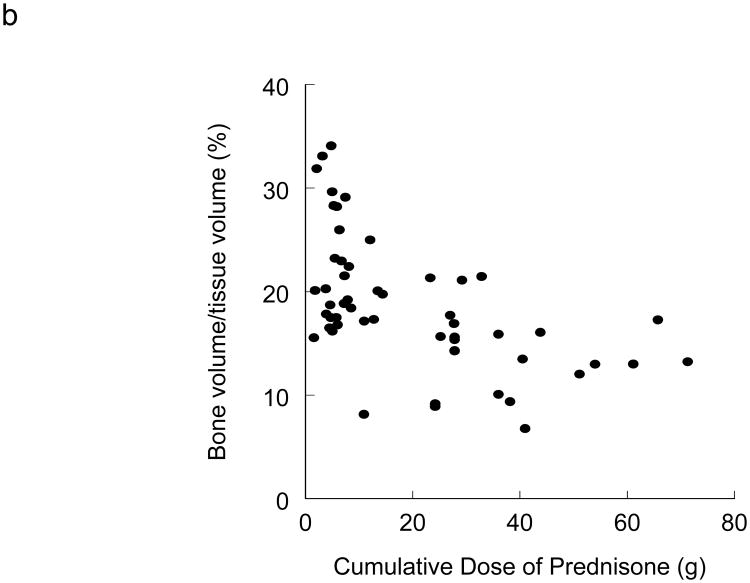
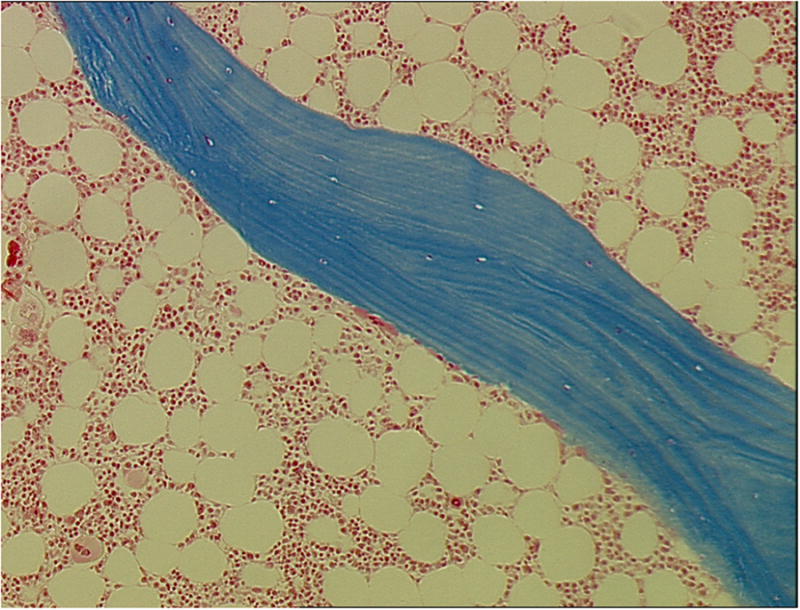
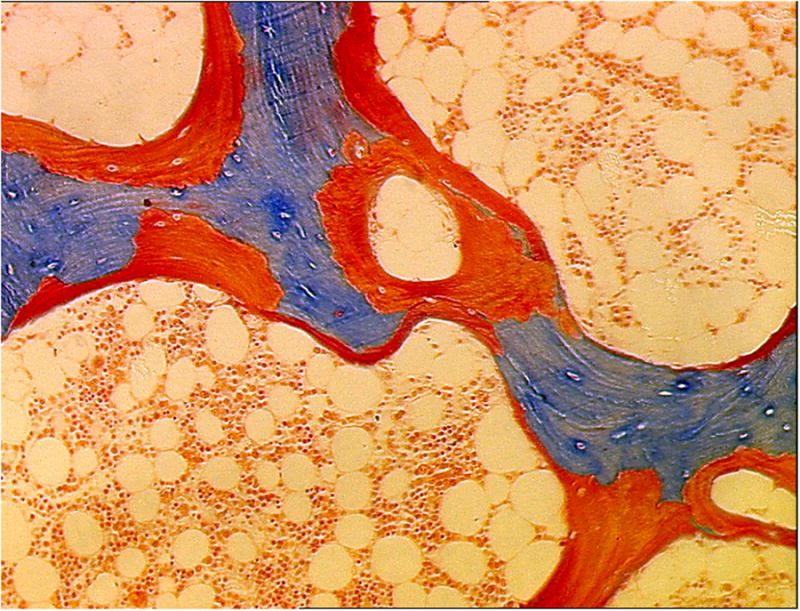
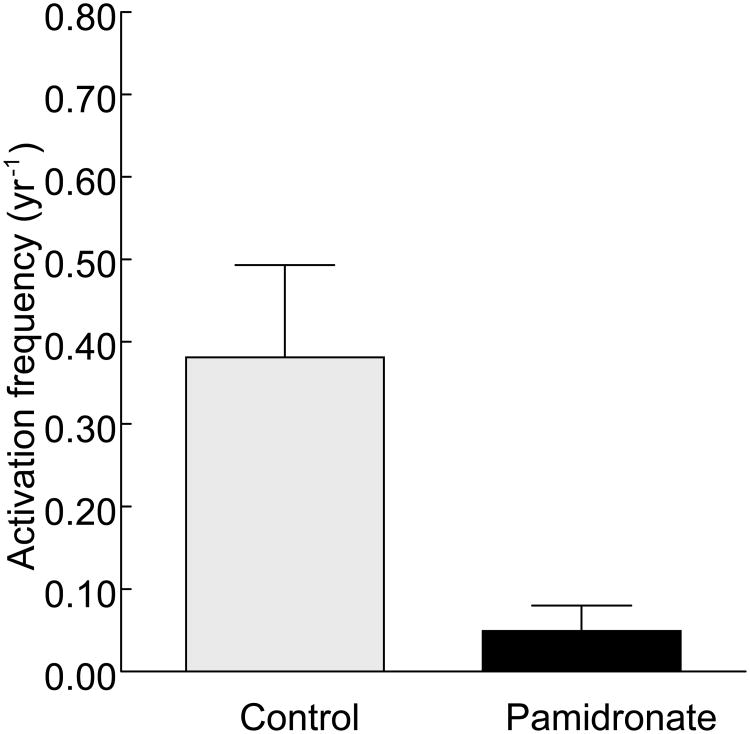
In light of greatly improved long-term patient and graft survival after renal transplantation, improving other clinical outcomes such as risk of fracture and cardiovascular disease is of paramount importance. After renal transplantation, a large percentage of patients lose bone. This loss of bone results from a combination of factors that include pre-existing renal osteodystrophy, immunosuppressive therapy, and the effects of chronically reduced renal function after transplantation. In addition to low bone volume, histological abnormalities include decreased bone turnover and defective mineralization. Low bone volume and low bone turnover were recently shown to be associated with cardiovascular calcifications, highlighting specific challenges for medical therapy and the need to prevent low bone turnover in the pretransplant patient. This Review discusses changes in bone histology and mineral metabolism that are associated with renal transplantation and the effects of these changes on clinical outcomes such as fractures and cardiovascular calcifications. Therapeutic modalities are evaluated based on our understanding of bone histology.
Figures

References
-
- Nishikawa K, Terasaki PI. Annual trends and triple therapy--1991-2000. Clin Transpl. 2001:247–69. - PubMed
-
- Marcen R, Teruel JL. Patient outcomes after kidney allograft loss. Transplant Rev (Orlando) 2008;22:62–72. - PubMed
-
- Malluche HH, Faugere MC. Atlas of Mineralized Bone Histology. Karger; New York: 1986.
-
- Hruska KA, Teitelbaum SL. Renal osteodystrophy. N Engl J Med. 1995;333:166–74. - PubMed
-
- Wang M, et al. Relationship between intact 1-84 parathyroid hormone and bone histomorphometric parameters in dialysis patients without aluminum toxicity. Am J Kidney Dis. 1995;26:836–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
