

Giant adrenal myelolipoma, a rare urological issue with increasing incidence: a case report
- PMID: 19918346
- PMCID: PMC2769476
- DOI: 10.4076/1757-1626-2-8863
Giant adrenal myelolipoma, a rare urological issue with increasing incidence: a case report
Abstract
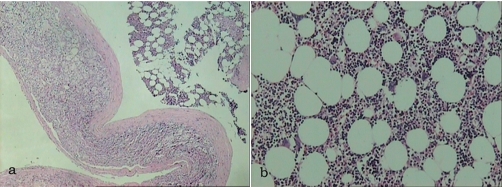
Introduction: Adrenal myelolipomas are relatively rare, non-functioning benign tumours composed of mature fatty and active hematopoietic elements. They can be asymptomatic, even if their size is massive. Diagnosis is relatively simple using ultrasound, computed tomography and magnetic resonance imaging. Surgical resection through an extraperitoneal approach is advocated in cases of symptomatic or large myelolipomas exceeding 5-cm in diameter. Their low incidence seems to be increasing from 0.2% to 10% during the last decade.
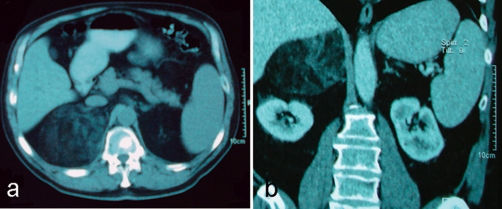
Case presentation: We present a case of a giant adrenal myelolipoma in a 68-year-old Caucasian male, who was presented with left lumbar pain. Renal ultrasound, CT and MRI demonstrated a well demarcated mass, with a maximum diameter of 10-cm. The differential diagnosis comprised the adrenal myelolipoma, the retroperitoneal liposarcoma and the renal angiomyolipoma. Thus, the patient was subjected to a left adrenalectomy.
Conclusion: Multiple theories have been proposed for the increasing frequency and natural course of the adrenal myelolipoma, with chronic adrenal stimulation and the contemporary stressful lifestyle to be the most appealing. Surgical treatment is advocated through an extraperitoneal approach because of the quicker recovery of the patient and the smaller postoperative complication rate.
Figures
Similar articles
-
Incidental detection of adrenal myelolipoma: a case report and review of literature.Case Rep Urol. 2013;2013:789481. doi: 10.1155/2013/789481. Epub 2013 Feb 20. Case Rep Urol. 2013. PMID: 23509660 Free PMC article.
-
Incidentally discovered adrenal myelolipoma. Report on 3 operated patients and update of the literature.Arch Ital Urol Androl. 2002 Sep;74(3):146-51. Arch Ital Urol Androl. 2002. PMID: 12416010 Review.
-
Robotic treatment of giant adrenal myelolipoma: A case report and review of the literature.Mol Clin Oncol. 2019 May;10(5):492-496. doi: 10.3892/mco.2019.1823. Epub 2019 Mar 12. Mol Clin Oncol. 2019. PMID: 31007910 Free PMC article.
-
Rare huge bilateral adrenal myelolipoma confused with retroperitoneal liposarcoma.IJU Case Rep. 2024 Oct 11;8(1):15-18. doi: 10.1002/iju5.12792. eCollection 2025 Jan. IJU Case Rep. 2024. PMID: 39749294 Free PMC article.
-
Asymptomatic bilateral giant adrenal myelolipomas: case report and review of literature.Endocr Pract. 2007 Oct;13(6):667-71. doi: 10.4158/EP.13.6.667. Endocr Pract. 2007. PMID: 17954426 Review.
Cited by
-
Non Functional Unilateral Adrenal Myelolipoma, A Case Report.J Clin Diagn Res. 2015 Jun;9(6):ED03-4. doi: 10.7860/JCDR/2015/13209.6070. Epub 2015 Jun 1. J Clin Diagn Res. 2015. PMID: 26266130 Free PMC article.
-
Coexistence of Myelolipoma and Primary Bilateral Macronodular Adrenal Hyperplasia With GIP-Dependent Cushing's Syndrome.Front Endocrinol (Lausanne). 2019 Sep 11;10:618. doi: 10.3389/fendo.2019.00618. eCollection 2019. Front Endocrinol (Lausanne). 2019. PMID: 31572300 Free PMC article.
-
Myelolipoma of the Pelvis: A Case Report and Review of Literature.Front Oncol. 2018 Jul 3;8:251. doi: 10.3389/fonc.2018.00251. eCollection 2018. Front Oncol. 2018. PMID: 30018883 Free PMC article.
-
Adrenal myelolipoma with osseous metaplasia and hypercortisolism.Urol Ann. 2017 Jan-Mar;9(1):71-73. doi: 10.4103/0974-7796.198841. Urol Ann. 2017. PMID: 28216934 Free PMC article.
-
Giant Adrenal Non-functioning Tumor: A Case Report and Review of Literature.Indian J Surg Oncol. 2012 Mar;3(1):30-2. doi: 10.1007/s13193-011-0109-z. Epub 2011 Dec 10. Indian J Surg Oncol. 2012. PMID: 23450947 Free PMC article. No abstract available.
References
-
- Settakorn J, Sirivanichai C, Rangdaeng S, Chaiwun B. Fine-needle aspiration cytology of adrenal myelolipoma: case report and review of the literature. Diagn Cytopathol. 1999;21:409–412. - PubMed
-
- Porcaro AB, Novella G, Ficarra V, Cavalleri S, Antoniolli SZ, Curti P. Incidentally discovered adrenal myelolipoma. Report on 3 operated patients and update of the literature. Arch Ital Urol Androl. 2002;74:146–151. - PubMed
-
- Vierna J, Laforga JB. Giant adrenal myelolipoma. Scand J Urol Nephrol. 1994;28:301–304. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
