

Mechanisms underlying skeletal muscle weakness in human heart failure: alterations in single fiber myosin protein content and function
- PMID: 19919996
- PMCID: PMC2782533
- DOI: 10.1161/CIRCHEARTFAILURE.109.876433
Mechanisms underlying skeletal muscle weakness in human heart failure: alterations in single fiber myosin protein content and function
Abstract
Background: Patients with chronic heart failure (HF) frequently experience skeletal muscle weakness that limits physical function. The mechanisms underlying muscle weakness, however, have not been clearly defined.
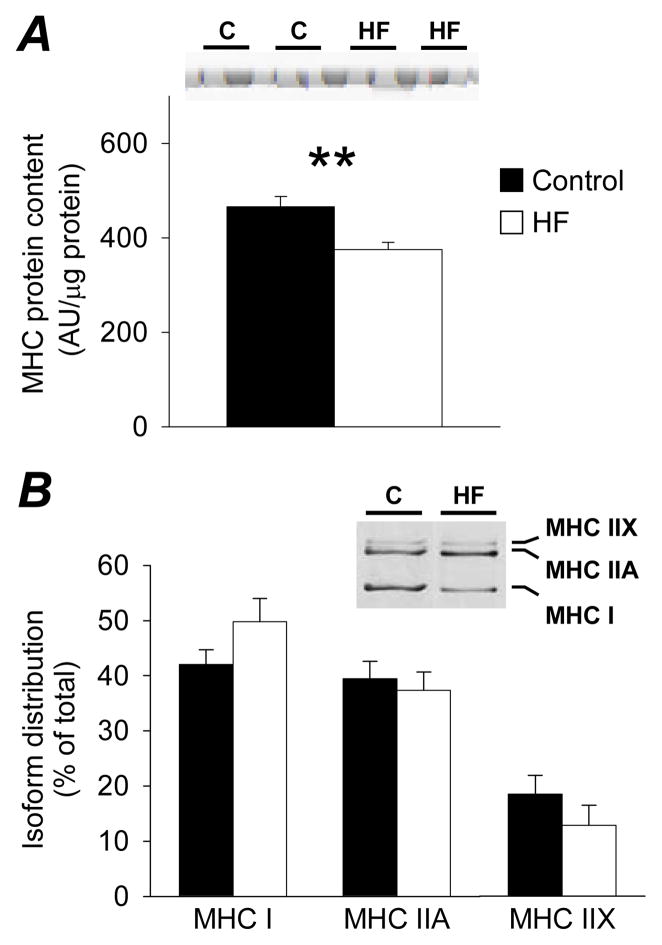
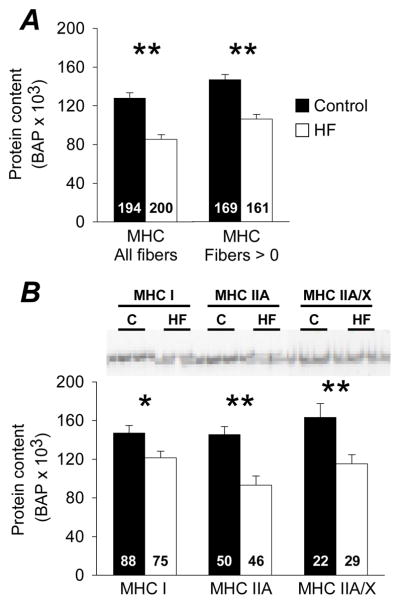
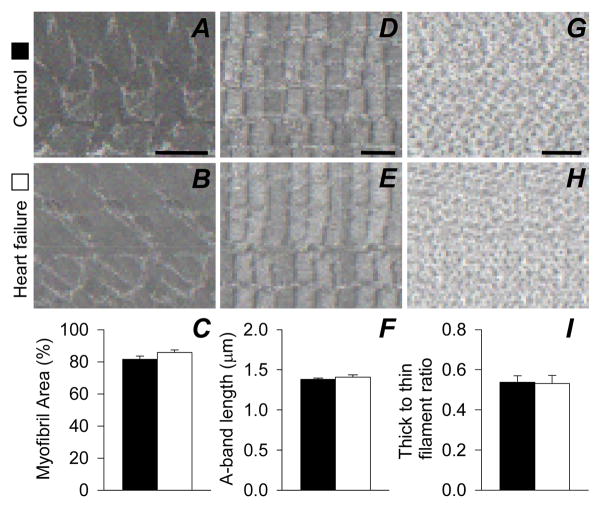
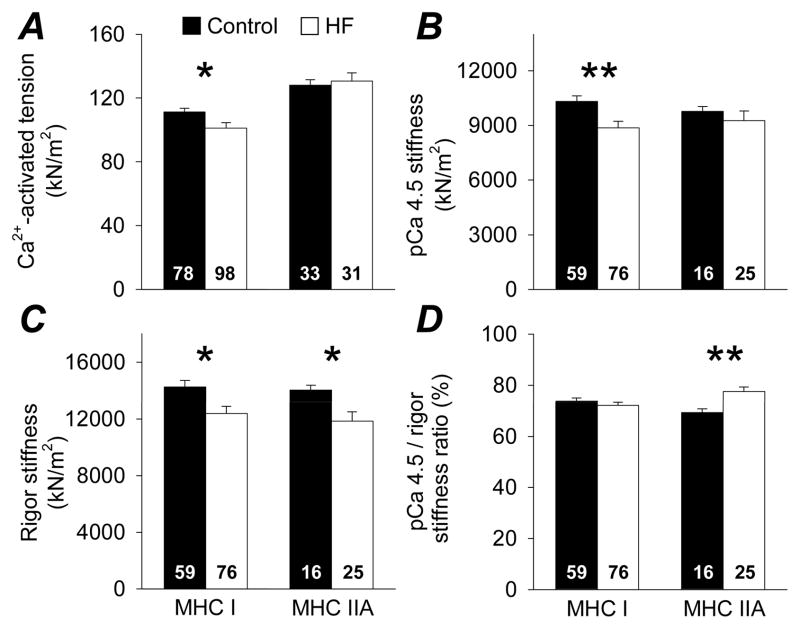
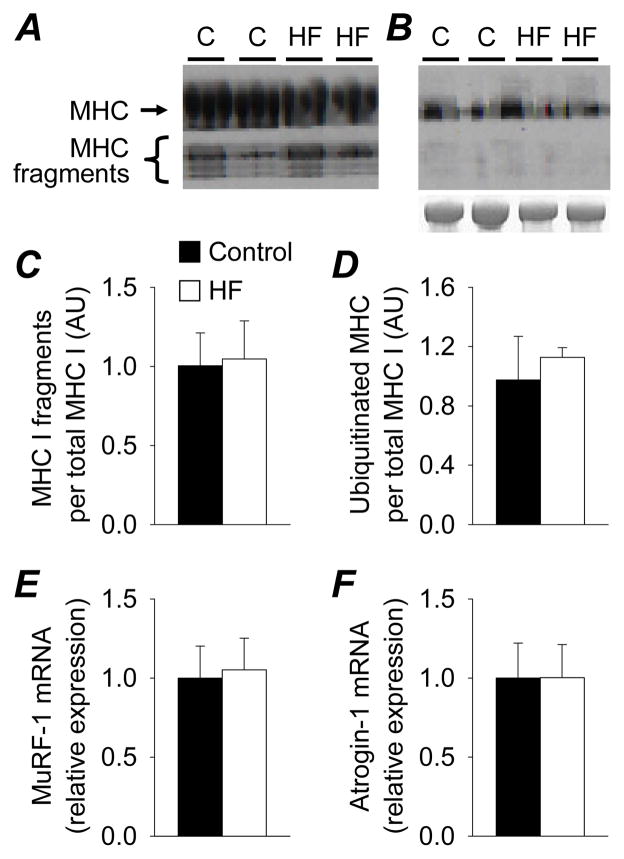
Methods and results: This study examined the hypothesis that HF promotes a loss of myosin protein from single skeletal muscle fibers, which in turn reduces contractile performance. Ten patients with chronic HF and 10 controls were studied. Muscle atrophy was not evident in patients, and groups displayed similar physical activity levels, suggesting that observed differences reflect the effects of HF and not muscle atrophy or disuse. In single muscle fibers, patients with HF showed reduced myosin heavy chain protein content (P<0.05) that manifested as a reduction in functional myosin-actin cross-bridges (P<0.05). No evidence was found for a generalized loss of myofilament protein, suggesting a selective loss of myosin. Accordingly, single muscle fiber maximal Ca(2+)-activated tension was reduced in myosin heavy chain I fibers in patients (P<0.05). However, tension was maintained in myosin heavy chain IIA fibers in patients because a greater proportion of available myosin heads were bound to actin during Ca(2+) activation (P<0.01).
Conclusions: Collectively, our results show that HF alters the quantity and functionality of the myosin molecule in skeletal muscle, leading to reduced tension in myosin heavy chain I fibers. Loss of single fiber myosin protein content represents a potential molecular mechanism underlying muscle weakness and exercise limitation in patients with HF.
Conflict of interest statement
No conflicts of interest to disclose.
Figures
Similar articles
-
Molecular mechanisms underlying skeletal muscle weakness in human cancer: reduced myosin-actin cross-bridge formation and kinetics.J Appl Physiol (1985). 2013 Apr;114(7):858-68. doi: 10.1152/japplphysiol.01474.2012. Epub 2013 Feb 14. J Appl Physiol (1985). 2013. PMID: 23412895 Free PMC article.
-
Chronic disuse and skeletal muscle structure in older adults: sex-specific differences and relationships to contractile function.Am J Physiol Cell Physiol. 2015 Jun 1;308(11):C932-43. doi: 10.1152/ajpcell.00014.2015. Epub 2015 Mar 25. Am J Physiol Cell Physiol. 2015. PMID: 25810256 Free PMC article.
-
Molecular determinants of force production in human skeletal muscle fibers: effects of myosin isoform expression and cross-sectional area.Am J Physiol Cell Physiol. 2015 Mar 15;308(6):C473-84. doi: 10.1152/ajpcell.00158.2014. Epub 2015 Jan 7. Am J Physiol Cell Physiol. 2015. PMID: 25567808 Free PMC article.
-
Age-related slowing of myosin actin cross-bridge kinetics is sex specific and predicts decrements in whole skeletal muscle performance in humans.J Appl Physiol (1985). 2013 Oct 1;115(7):1004-14. doi: 10.1152/japplphysiol.00563.2013. Epub 2013 Jul 25. J Appl Physiol (1985). 2013. PMID: 23887900 Free PMC article.
-
Making the case for skeletal myopathy as the major limitation of exercise capacity in heart failure.Circ Heart Fail. 2010 Jul;3(4):537-46. doi: 10.1161/CIRCHEARTFAILURE.109.903773. Circ Heart Fail. 2010. PMID: 20647489 Free PMC article. Review. No abstract available.
Cited by
-
Impact of whole-body and skeletal muscle composition on peak oxygen uptake in heart failure: a systematic review and meta-analysis.Eur Heart J Open. 2024 Sep 26;4(5):oeae082. doi: 10.1093/ehjopen/oeae082. eCollection 2024 Sep. Eur Heart J Open. 2024. PMID: 39464232 Free PMC article.
-
Influenza Infection has Fiber Type-Specific Effects on Cellular and Molecular Skeletal Muscle Function in Aged Mice.J Gerontol A Biol Sci Med Sci. 2020 Nov 13;75(12):2333-2341. doi: 10.1093/gerona/glaa136. J Gerontol A Biol Sci Med Sci. 2020. PMID: 32492709 Free PMC article.
-
Muscle disuse alters skeletal muscle contractile function at the molecular and cellular levels in older adult humans in a sex-specific manner.J Physiol. 2014 Oct 15;592(20):4555-73. doi: 10.1113/jphysiol.2014.279034. Epub 2014 Jul 18. J Physiol. 2014. PMID: 25038243 Free PMC article.
-
Muscular changes in animal models of heart failure with preserved ejection fraction: what comes closest to the patient?ESC Heart Fail. 2021 Feb;8(1):139-150. doi: 10.1002/ehf2.13142. Epub 2020 Dec 17. ESC Heart Fail. 2021. PMID: 33350094 Free PMC article.
-
Utility of Neuromuscular Electrical Stimulation to Preserve Quadriceps Muscle Fiber Size and Contractility After Anterior Cruciate Ligament Injuries and Reconstruction: A Randomized, Sham-Controlled, Blinded Trial.Am J Sports Med. 2020 Aug;48(10):2429-2437. doi: 10.1177/0363546520933622. Epub 2020 Jul 6. Am J Sports Med. 2020. PMID: 32631074 Free PMC article. Clinical Trial.
References
-
- Toth MJ, Gottlieb SS, Fisher ML, Poehlman ET. Skeletal muscle atrophy and peak oxygen consumption in heart failure. Am J Cardiol. 1997;79:1267–1269. - PubMed
-
- Harrington D, Anker SD, Chua TP, Webb-Peploe KM, Ponikowski PP, Poole-Wilson PA, Coats AJ. Skeletal muscle function and its relation to exercise tolerance in chronic heart failure. J Am Coll Cardiol. 1997;30:1758–1764. - PubMed
-
- Minotti JR, Pillay P, Chang L, Wells L, Massie BM. Neurophysiological assessment of skeletal muscle fatigue in patients with congestive heart failure. Circulation. 1992;86:903–908. - PubMed
-
- Wilson JR, Mancini DM. Factors contributing to the exercise limitation of heart failure. J Am Coll Cardiol. 1993;22:93A–98A. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
