

The Bypass Angioplasty Revascularization Investigation 2 Diabetes randomized trial of different treatment strategies in type 2 diabetes mellitus with stable ischemic heart disease: impact of treatment strategy on cardiac mortality and myocardial infarction
- PMID: 19920001
- PMCID: PMC2830563
- DOI: 10.1161/CIRCULATIONAHA.109.913111
The Bypass Angioplasty Revascularization Investigation 2 Diabetes randomized trial of different treatment strategies in type 2 diabetes mellitus with stable ischemic heart disease: impact of treatment strategy on cardiac mortality and myocardial infarction
Erratum in
- Circulation. 2010 Mar 30;121(12):e254
Abstract
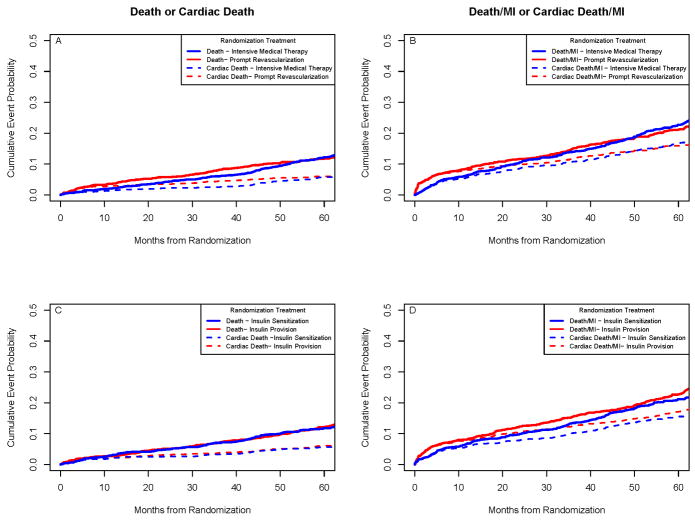
Background: The Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) trial in 2368 patients with stable ischemic heart disease assigned before randomization to percutaneous coronary intervention or coronary artery bypass grafting strata reported similar 5-year all-cause mortality rates with insulin sensitization versus insulin provision therapy and with a strategy of prompt initial coronary revascularization and intensive medical therapy or intensive medical therapy alone with revascularization reserved for clinical indication(s). In this report, we examine the predefined secondary end points of cardiac death and myocardial infarction (MI).
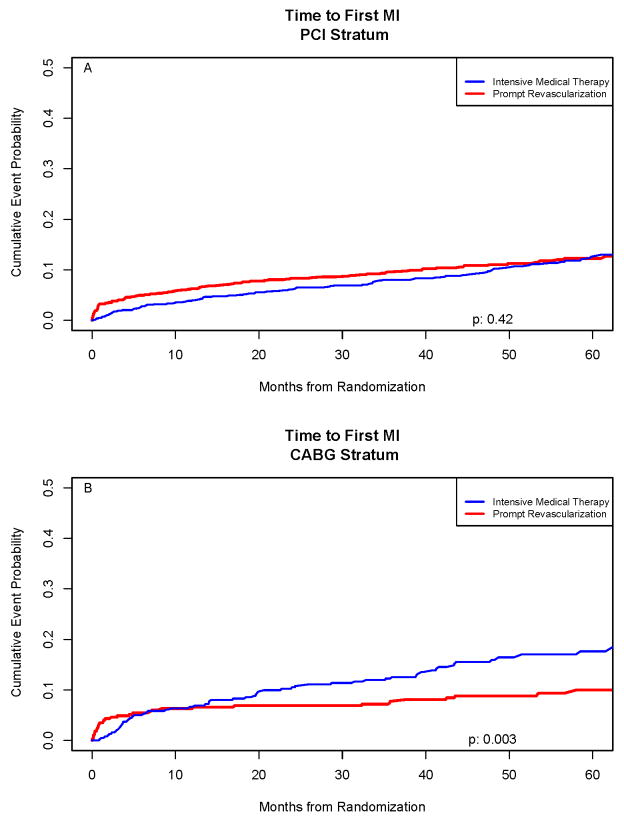
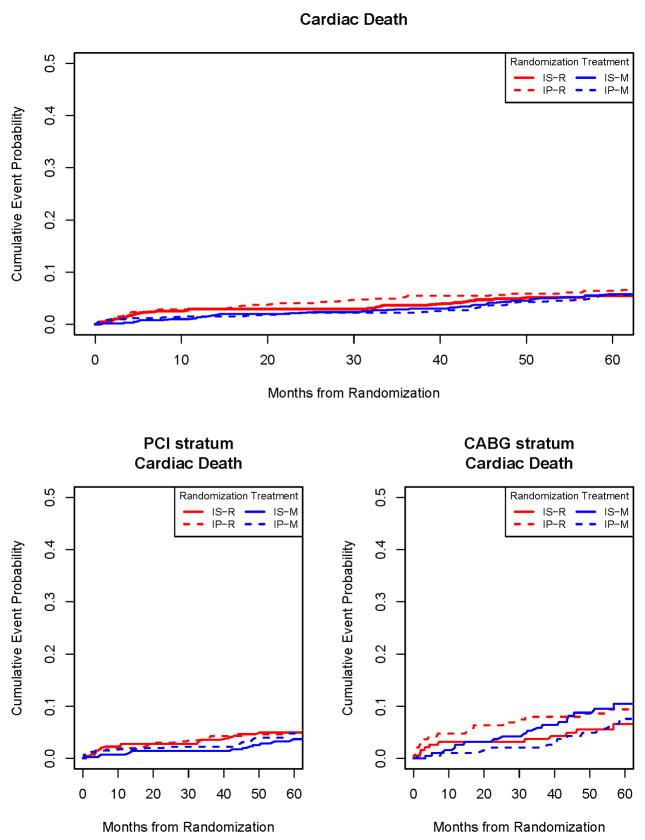
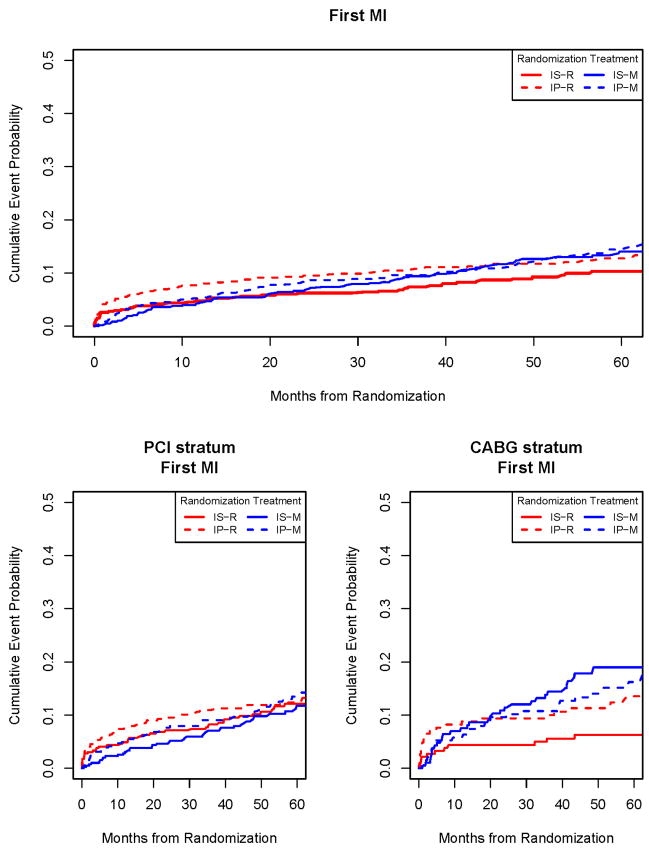
Methods and results: Outcome data were analyzed by intention to treat; the Kaplan-Meier method was used to assess 5-year event rates. Nominal P values are presented. During an average 5.3-year follow-up, there were 316 deaths (43% were attributed to cardiac causes) and 279 first MI events. Five-year cardiac mortality did not differ between revascularization plus intensive medical therapy (5.9%) and intensive medical therapy alone groups (5.7%; P=0.38) or between insulin sensitization (5.7%) and insulin provision therapy (6%; P=0.76). In the coronary artery bypass grafting stratum (n=763), MI events were significantly less frequent in revascularization plus intensive medical therapy versus intensive medical therapy alone groups (10.0% versus 17.6%; P=0.003), and the composite end points of all-cause death or MI (21.1% versus 29.2%; P=0.010) and cardiac death or MI (P=0.03) were also less frequent. Reduction in MI (P=0.001) and cardiac death/MI (P=0.002) was significant only in the insulin sensitization group.
Conclusions: In many patients with type 2 diabetes mellitus and stable ischemic coronary disease in whom angina symptoms are controlled, similar to those enrolled in the percutaneous coronary intervention stratum, intensive medical therapy alone should be the first-line strategy. In patients with more extensive coronary disease, similar to those enrolled in the coronary artery bypass grafting stratum, prompt coronary artery bypass grafting, in the absence of contraindications, intensive medical therapy, and an insulin sensitization strategy appears to be a preferred therapeutic strategy to reduce the incidence of MI.
Trial registration: ClinicalTrials.gov NCT00006305.
Conflict of interest statement
Dr. Chaitman reports receiving consulting/advisory board fees from Eli Lilly and lecture fees from Gilead. No other potential conflict of interest relevant to this article was reported.
Figures

References
-
- Stevens RJ, Kothari V, Adler AI, Stratton IM, Holman RR on behalf of the United Kingdom Prospective Diabetes Study (UKPDS) Group. The UKPDS risk engine: a model for the risk of coronary heart disease in Type II diabetes (UKPDS 56) Clin Sci. 2001;101:671–679. - PubMed
-
- Franco OH, Steyerberg EW, Hu FB, Mackenbach J, Nusselder W. Association of diabetes mellitus with total life expectancy and life expectancy with and without cardiovascular disease. Arch Intern Med. 2007;167:1145–1151. - PubMed
-
- Geiss LS, Herman WH, Smith PJ. Mortality in non-insulin-dependent diabetes. In: Aubert RE, Ballard DJ, Barrett-Connor E, et al., editors. Diabetes in America. 2. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases; 1995. pp. 233–57. (NIH publication no. 95-1468.)
-
- Barsness GW, Gersh BJ, Brooks MM, Frye RL. Rationale for the revascularization arm of the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) Trial. Am J Cardiol. 2006;97(Suppl 12A):31G–40G. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
