

Hypertension improvement project: randomized trial of quality improvement for physicians and lifestyle modification for patients
- PMID: 19920081
- PMCID: PMC2784648
- DOI: 10.1161/HYPERTENSIONAHA.109.134874
Hypertension improvement project: randomized trial of quality improvement for physicians and lifestyle modification for patients
Abstract
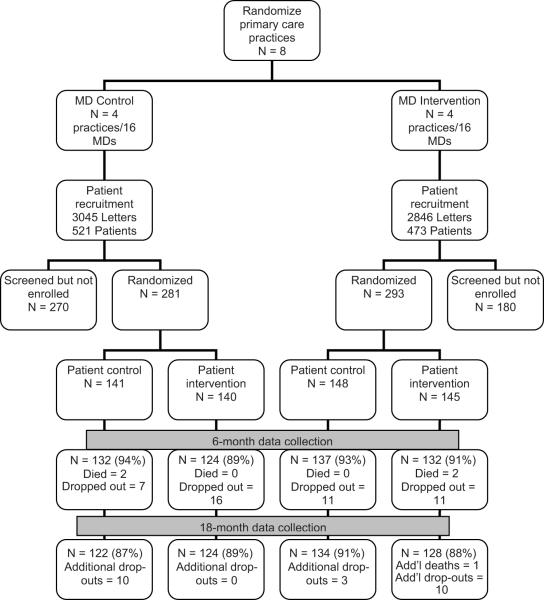
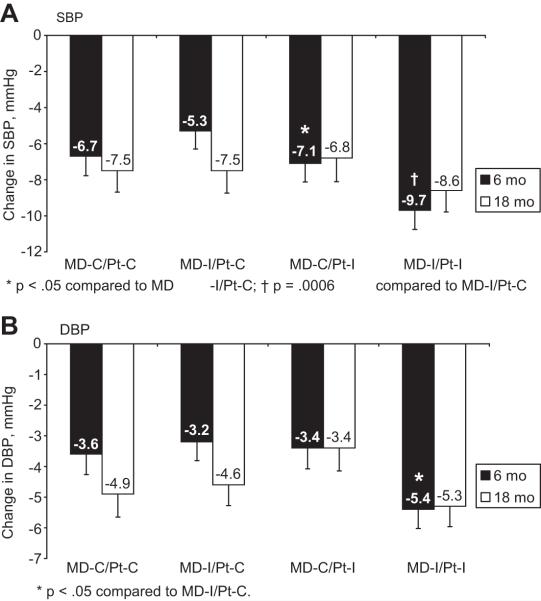
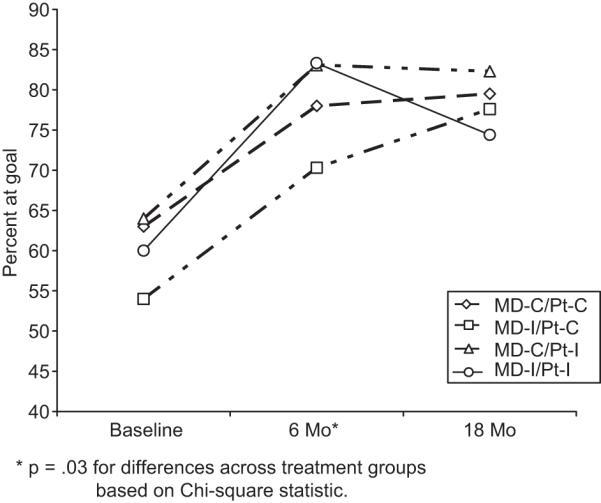
Despite widely publicized hypertension treatment guidelines for physicians and lifestyle recommendations for patients, blood pressure control rates remain low. In community-based primary care clinics, we performed a nested, 2 x 2 randomized, controlled trial of physician intervention versus control and/or patient intervention versus control. Physician intervention included internet-based training, self-monitoring, and quarterly feedback reports. Patient intervention included 20 weekly group sessions followed by 12 monthly telephone counseling contacts and focused on weight loss, Dietary Approaches to Stop Hypertension dietary pattern, exercise, and reduced sodium intake. The primary outcome was change in systolic blood pressure at 6 months. Eight primary care practices (32 physicians) were randomized to physician intervention or control groups. Within those practices, 574 patients were randomized to patient intervention or control groups. Patient mean age was 60 years, 61% were women, and 37% were black. Blood pressure data were available for 91% of patients at 6 months. The main effect of physician intervention on systolic blood pressure at 6 months, adjusted for baseline pressure, was 0.3 mm Hg (95% CI: 1.5 to 2.2; P=0.72). The main effect of the patient intervention was 2.6 mm Hg (95% CI: 4.4 to 0.7; P=0.01). The interaction of the 2 interventions was significant (P=0.03); the largest impact was observed with the combination of physician and patient intervention (9.7 +/- 12.7 mm Hg). Differences between treatment groups did not persist at 18 months. Combined physician and patient interventions lowers blood pressure; future research should focus on enhancing effectiveness and sustainability of these interventions.
Trial registration: ClinicalTrials.gov NCT00201136.
Figures
Comment in
-
Both the toolset and motivation are needed for lasting change.Hypertension. 2009 Dec;54(6):1202-3. doi: 10.1161/HYPERTENSIONAHA.109.139584. Hypertension. 2009. PMID: 19920080 No abstract available.
-
Synergistic physician and patient behavioral interventions as management strategy for effective population-based hypertension control.Curr Hypertens Rep. 2010 Jun;12(3):149-51. doi: 10.1007/s11906-010-0111-9. Curr Hypertens Rep. 2010. PMID: 20424947 Free PMC article. No abstract available.
References
-
- Working Group Report on Primary Prevention of Hypertension . National High Blood Pressure Education Program. National Institutes of Health, National Heart, Lung, and Blood Institutes document Bethesda: National Institutes of Health; 2000.
-
- Kannel WB. Blood pressure as a cardiovascular risk factor: prevention and treatment. Journal of the American Medical Association. 1996;275:1571–1576. - PubMed
-
- Psaty B, Smith NL, Siscovick DS, Koepsell TD, Weiss NS, Heckbert SR, Lemaitre RN, Wagner EH, Furberg CD. Health outcomes associated with anti-hypertensive therapies used as first line agents: A systematic review and meta-analysis. Journal of the American Medical Association. 1997;277:739–745. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr., Jones DW, Materson BJ, Oparil S, Wright JT, Jr., Roccella EJ. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. Hypertension. 2003;42:1206–1252. - PubMed
-
- Singer GM, Izhar M, Black HR. Guidelines for hypertension: are quality-assurance measures on target? Hypertension. 2004;43:198–202. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
