

DOES MEDICARE SAVE LIVES?
- PMID: 19920880
- PMCID: PMC2777733
- DOI: 10.1162/qjec.2009.124.2.597
DOES MEDICARE SAVE LIVES?
Abstract
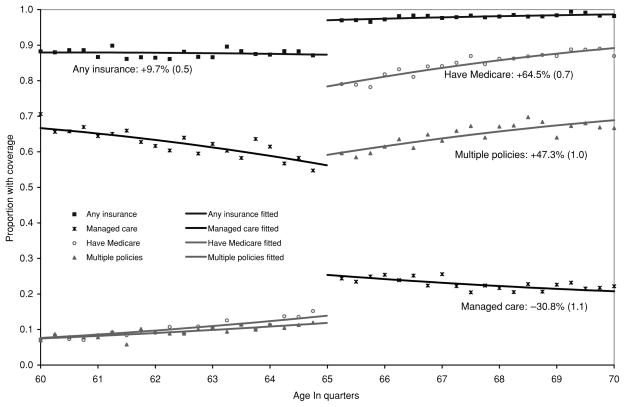
Health insurance characteristics shift at age 65 as most people become eligible for Medicare. We measure the impacts of these changes on patients who are admitted to hospitals through emergency departments for conditions with similar admission rates on weekdays and weekends. The age profiles of admissions and comorbidities for these patients are smooth at age 65, suggesting that the severity of illness is similar on either side of the Medicare threshold. In contrast, the number of procedures performed in hospitals and total list charges exhibit small but statistically significant discontinuities, implying that patients over 65 receive more services. We estimate a nearly 1-percentage-point drop in 7-day mortality for patients at age 65, equivalent to a 20% reduction in deaths for this severely ill patient group. The mortality gap persists for at least 9 months after admission.
Figures






References
-
- Autor David H, Duggan Mark G. The Rise in the Disability Rolls and the Decline in Unemployment. Quarterly Journal of Economics. 2003;118:157–205.
-
- Canto John G, Rogers William J, Chandra Nisha C, French William J, Barron Hal V, Frederick Paul D, Maynard Charles, Every Nathan R. The Association of Sex and Payer Status on Management and Subsequent Survival in Acute Myocardial Infarction. Archives of Internal Medicine. 2000;162:587–593. - PubMed
-
- Cohen Robin A, Martinez Michael E. Impact of Medicare and Medicaid Probe Questions on Health Insurance Estimates in the National Health Interview Survey, 2005. Report, Centers for Disease Control, National Center for Health Statistics. 2007 May;
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous