

The phenotypic spectrum of contiguous deletion of CYP21A2 and tenascin XB: quadricuspid aortic valve and other midline defects
- PMID: 19921645
- PMCID: PMC2963110
- DOI: 10.1002/ajmg.a.33092
The phenotypic spectrum of contiguous deletion of CYP21A2 and tenascin XB: quadricuspid aortic valve and other midline defects
Abstract
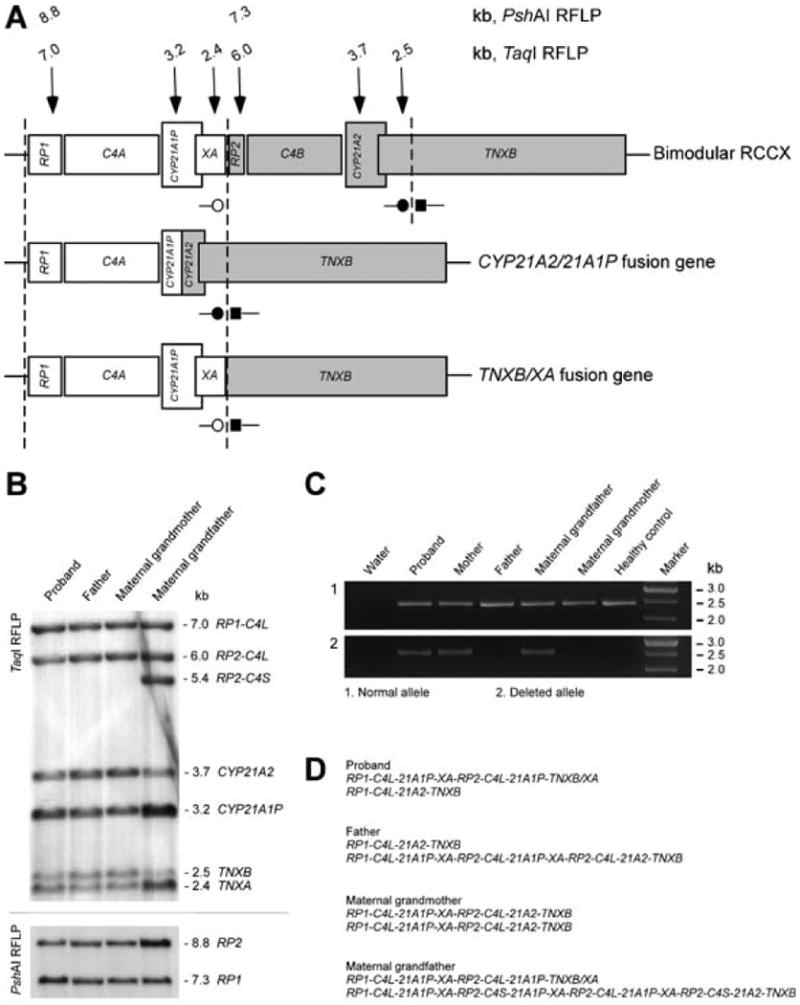
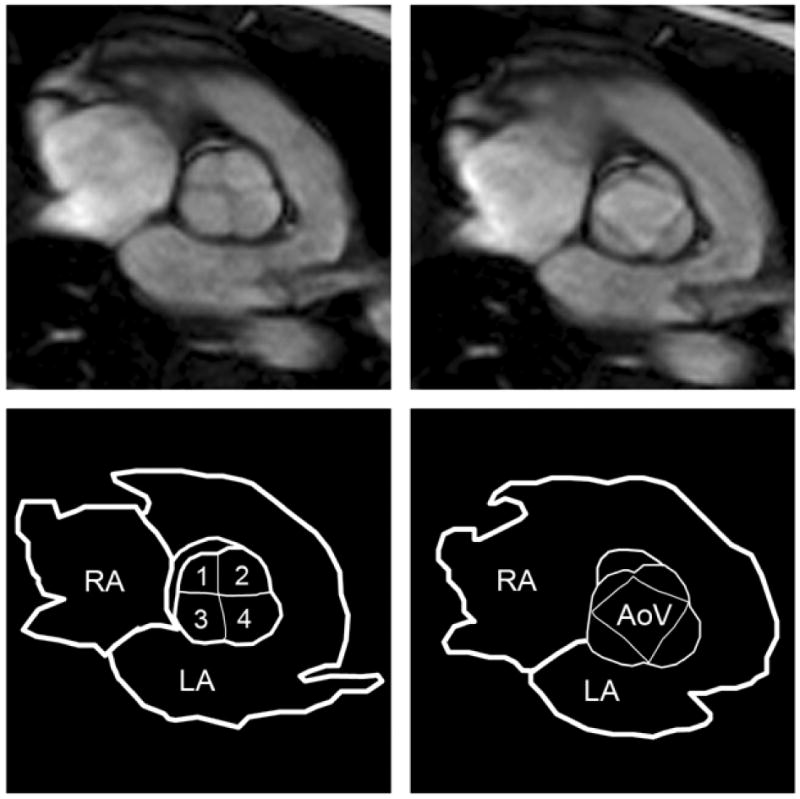
Congenital adrenal hyperplasia (CAH) due to 21-hydroxylase deficiency is an autosomal recessive disorder and is the most common cause of ambiguous genitalia in the newborn. The genes encoding 21-hydroxylase, CYP21A2, and tenascin-X (TNX), TNXB, are located within the HLA complex, in a region of high gene density termed the RCCX module. The module has multiple pseudogenes as well as tandem repeat sequences that promote misalignment during meiosis leading to complex gene rearrangements, deletions and gene conversion events. CYP21A2 mutations cause CAH, and TNX deficiency has been identified as a cause of hypermobility type Ehlers-Danlos syndrome (EDS). Here we report on a three-generation family with a heterozygous deletion encompassing CYP21A2 and TNXB that initially came to medical attention due to the diagnosis of CAH in the proposita. Southern blotting and PCR-based analysis of the RCCX module revealed a CYP21A2 deletion extending into TNXB in one allele and a CYP21A2 point mutation in the other allele. Family history is notable for joint hypermobility. Additional radiological and clinical investigations showed a quadricuspid aortic valve, single kidney, bicornuate uterus and a bifid uvula in the proposita, and mitral valve prolapse in her mother. These findings further delineate the phenotype of the CAH-TNX contiguous gene deletion syndrome and point to an intersection of connective tissue dysplasias with a common gene-mediated endocrine disorder.
Figures
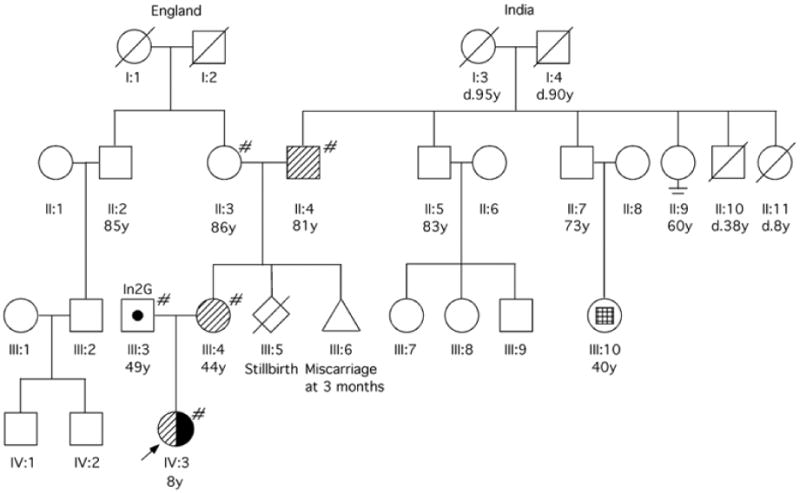
 Carrier of TNXB/XA fusion gene (CYP21A2 deletion);
Carrier of TNXB/XA fusion gene (CYP21A2 deletion);  Carrier of CYP21A2 point mutation (In2G);
Carrier of CYP21A2 point mutation (In2G);  Affected by CAH, compound heterozygote (TNXB/XA, In2G).
Affected by CAH, compound heterozygote (TNXB/XA, In2G).  Facial asymmetry with ipsilateral ear dysplasia and unilateral deafness, but normal intelligence.
Facial asymmetry with ipsilateral ear dysplasia and unilateral deafness, but normal intelligence.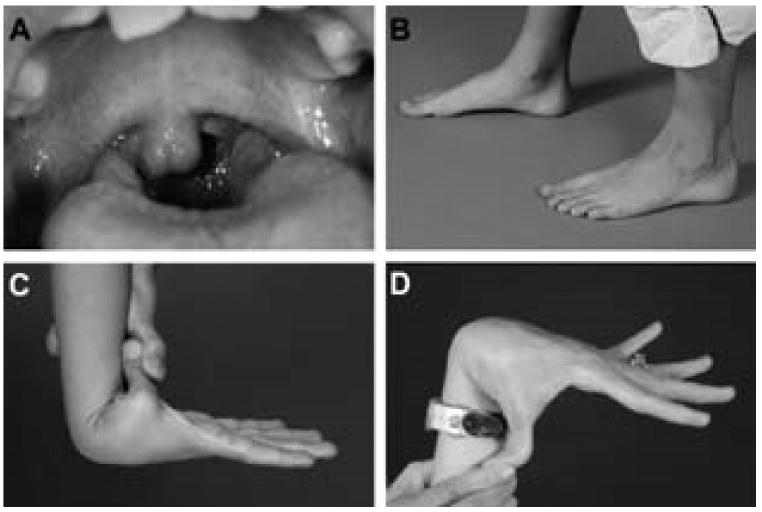
Similar articles
-
Measurement of serum tenascin-X in patients with congenital adrenal hyperplasia at risk for Ehlers-Danlos contiguous gene deletion syndrome CAH-X.BMC Res Notes. 2019 Oct 30;12(1):711. doi: 10.1186/s13104-019-4753-7. BMC Res Notes. 2019. PMID: 31666125 Free PMC article.
-
Tenascin-X haploinsufficiency associated with Ehlers-Danlos syndrome in patients with congenital adrenal hyperplasia.J Clin Endocrinol Metab. 2013 Feb;98(2):E379-87. doi: 10.1210/jc.2012-3148. Epub 2013 Jan 2. J Clin Endocrinol Metab. 2013. PMID: 23284009 Free PMC article.
-
A TNXB splice donor site variant as a cause of hypermobility type Ehlers-Danlos syndrome in patients with congenital adrenal hyperplasia.Mol Genet Genomic Med. 2021 Feb;9(2):e1556. doi: 10.1002/mgg3.1556. Epub 2020 Dec 17. Mol Genet Genomic Med. 2021. PMID: 33332743 Free PMC article.
-
Tenascin-X, Congenital Adrenal Hyperplasia, and the CAH-X Syndrome.Horm Res Paediatr. 2018;89(5):352-361. doi: 10.1159/000481911. Epub 2018 May 7. Horm Res Paediatr. 2018. PMID: 29734195 Free PMC article. Review.
-
Congenital Adrenal Hyperplasia and Ehlers-Danlos Syndrome.Front Endocrinol (Lausanne). 2022 Feb 25;13:803226. doi: 10.3389/fendo.2022.803226. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35282436 Free PMC article. Review.
Cited by
-
Extracellular Matrix Remodeling During Palate Development.Organogenesis. 2020 Apr 2;16(2):43-60. doi: 10.1080/15476278.2020.1735239. Epub 2020 Mar 31. Organogenesis. 2020. PMID: 32233728 Free PMC article. Review.
-
Genetic risk factors for eating disorders: an update and insights into pathophysiology.Ther Adv Psychopharmacol. 2019 Feb 12;9:2045125318814734. doi: 10.1177/2045125318814734. eCollection 2019. Ther Adv Psychopharmacol. 2019. PMID: 30800283 Free PMC article. Review.
-
Long-Read Sequencing Identifying the Genetic Complexity of Congenital Adrenal Hyperplasia in the Pedigree.Mol Genet Genomic Med. 2024 Nov;12(11):e70029. doi: 10.1002/mgg3.70029. Mol Genet Genomic Med. 2024. PMID: 39575462 Free PMC article.
-
Genetics of congenital adrenal hyperplasia.Best Pract Res Clin Endocrinol Metab. 2009 Apr;23(2):181-92. doi: 10.1016/j.beem.2008.10.014. Best Pract Res Clin Endocrinol Metab. 2009. PMID: 19500762 Free PMC article. Review.
-
High-Throughput Screening for CYP21A1P-TNXA/TNXB Chimeric Genes Responsible for Ehlers-Danlos Syndrome in Patients with Congenital Adrenal Hyperplasia.J Mol Diagn. 2019 Sep;21(5):924-931. doi: 10.1016/j.jmoldx.2019.06.001. Epub 2019 Jun 21. J Mol Diagn. 2019. PMID: 31229653 Free PMC article.
References
-
- Armen TA, Vandse R, Bickle K, Nathan N. Three-dimensional echocardiographic evaluation of an incidental quadricuspid aortic valve. Eur J Echocardiogr. 2008;9(2):318–20. - PubMed
-
- Beighton P, De Paepe A, Steinmann B, Tsipouras P, Wenstrup RJ. Ehlers-Danlos syndromes: revised nosology, Villefranche, 1997. Ehlers-Danlos National Foundation (USA) and Ehlers-Danlos Support Group (UK) Am J Med Genet. 1998;77(1):31–7. - PubMed
-
- Bristow J, Carey W, Egging D, Schalkwijk J. Tenascin-X, collagen, elastin, and the Ehlers-Danlos syndrome. Am J Med Genet C Semin Med Genet. 2005;139C(1):24–30. - PubMed
-
- Burch GH, Bedolli MA, McDonough S, Rosenthal SM, Bristow J. Embryonic expression of tenascin-X suggests a role in limb, muscle, and heart development. Dev Dyn. 1995;203(4):491–504. - PubMed
-
- Burch GH, Gong Y, Liu W, Dettman RW, Curry CJ, Smith L, Miller WL, Bristow J. Tenascin-X deficiency is associated with Ehlers-Danlos syndrome. Nat Genet. 1997;17(1):104–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
