

Cost-effectiveness of postural exercise therapy versus physiotherapy in computer screen-workers with early non-specific work-related upper limb disorders (WRULD); a randomized controlled trial
- PMID: 19922603
- PMCID: PMC2785778
- DOI: 10.1186/1745-6215-10-103
Cost-effectiveness of postural exercise therapy versus physiotherapy in computer screen-workers with early non-specific work-related upper limb disorders (WRULD); a randomized controlled trial
Abstract
Background: Exercise therapies generate substantial costs in computer workers with non-specific work-related upper limb disorders (WRULD).
Aims: To study if postural exercise therapy is cost-effective compared to regular physiotherapy in screen-workers with early complaints, both from health care and societal perspective.
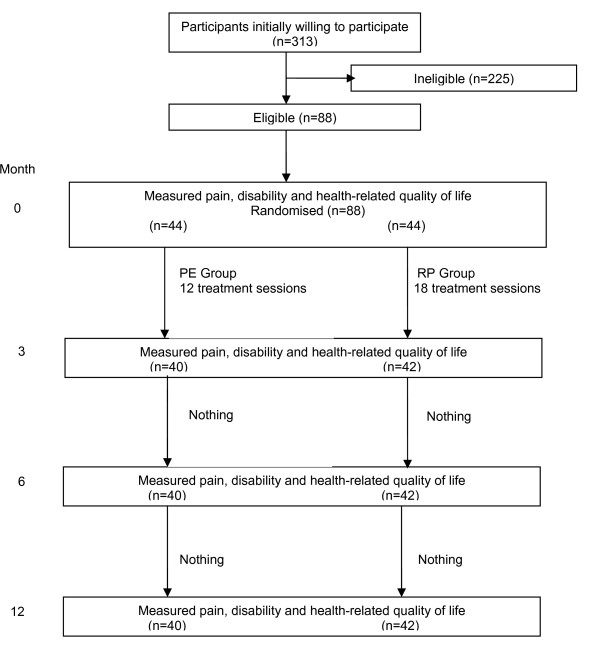
Methods: Prospective randomized trial including cost-effectiveness analysis; one year follow-up.
Participants: Eighty-eight screen-workers with early non-specific WRULD; six drop-outs.
Interventions: A ten week postural exercise program versus regular physiotherapy.
Outcome measures: Effectiveness measures: Pain: visual analogous scale (VAS), self-perceived WRULD (yes/no). Functional outcome: Disabilities of Arm, Shoulder and Hand- Dutch Language Version (DASH-DLV). Quality of life outcome: EQ-5D.Economic measures: health care costs including patient and family costs and productivity costs resulting in societal costs. Cost-effectiveness measures: health care costs and societal costs related to the effectiveness measures. OUTCOME MEASURES were assessed at baseline; three, six and twelve months after baseline.
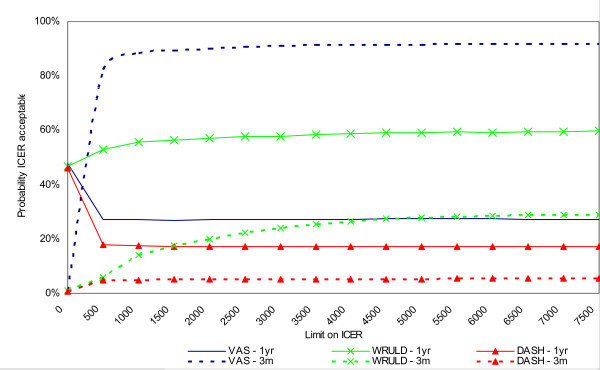
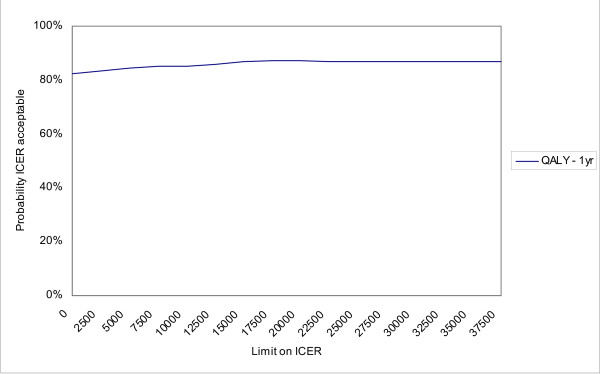
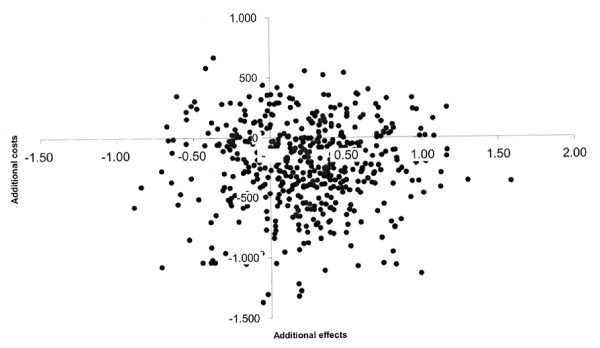
Results: At baseline both groups were comparable for baseline characteristics except scores on the Pain Catastrophizing Scale and comparable for costs. No significant differences between the groups concerning effectiveness at one year follow-up were found. Effectiveness scores slightly improved over time. After one year 55% of participants were free of complaints. After one year the postural exercise group had higher mean total health care costs, but lower productivity costs compared to the physiotherapy group. Mean societal costs after one year (therefore) were in favor of postural exercise therapy [- euro622; 95% CI -2087; +590)]. After one year, only self- perceived WRULD seemed to result in acceptable cost-effectiveness of the postural exercise strategy over physiotherapy; however the probability of acceptable cost-effectiveness did not exceed 60%.Considering societal costs related to QALYs, postural exercise therapy had a probability of over 80% to be cost-effective over a wide range of cost-effectiveness ceiling ratios; however based on a marginal QALY-difference of 0.1 over a 12 month time frame.
Conclusion: Although our trial failed to find significant differences in VAS, QALYs and ICERs based on VAS and QALYs at one-year follow-up, CEACs suggest that postural exercise therapy according to Mensendieck/Cesar has a higher probability of being cost-effective compared to regular physiotherapy; however further research is required.
Trial registration: ISRCTN 15872455.
Figures
References
-
- RSI. The Hague: Health Council of the Netherlands; Publication No. 2000/22E. http://neurologiadeltrabajo.sen.es/pdf/rsi_report_curso2000_nt.pdf Retrieved November 1, 2005.
-
- Peereboom KJ. RSI Handboek (RSI Handbook) 4. The Hague, the Netherlands: Sdu Editors; 2005.
-
- Gezondheidsschade en kosten als gevolg van RSI en psychosociale arbeidsbelasting in Nederland. (Health effects and costs as consequences of RSI and psychosocial work load in the Netherlands). TNO Kwaliteit van Leven/Ministerie van Sociale Zaken en Werkgelegenheid. 2005. http://docs.szw.nl/pdf/129/2006/129_2006_3_8656.pdf Retrieved October 28, 2005,
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
